We grow taller because specialized cartilage zones at the ends of our long bones, called growth plates, keep producing new bone tissue throughout childhood and adolescence. Cells in those plates multiply, expand, and eventually mineralize into solid bone, pushing the skeleton longer with each cycle. The whole process is orchestrated by growth hormone, IGF-1, thyroid hormone, and sex steroids, and it stops permanently once those plates fuse, typically in the late teens to early twenties. After that, no supplement, stretch, or exercise can reopen them.
Why Do We Grow Taller? Science, Hormones, and What Helps

Marcus Reeves
12 Jun 2026

How height growth actually works in the body

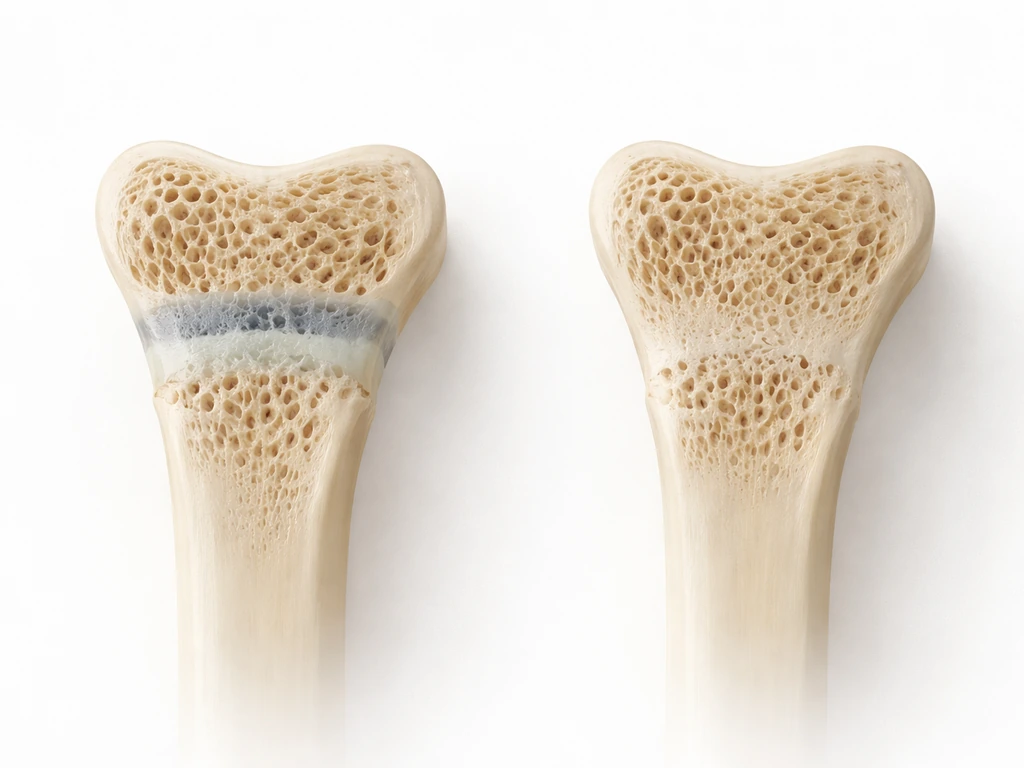
The growth plate, or physis, sits near each end of the long bones in your legs and arms. It is made of cartilage organized into distinct zones. In the proliferative zone, chondrocytes (cartilage cells) divide rapidly. They then move into the hypertrophic zone, where they swell dramatically in size. Research identifies that enlargement of hypertrophic chondrocytes is one of the biggest single contributors to how fast a bone actually gets longer. After the cells reach their maximum size, the surrounding matrix mineralizes and becomes true bone, and the cycle repeats. The faster this cycle runs, the faster you grow.
The endocrine system controls the pace of all of this. Growth hormone (GH), released in pulses from the pituitary gland, triggers the liver to produce IGF-1 (insulin-like growth factor 1), which acts directly on growth plate chondrocytes to stimulate both proliferation and hypertrophy. Clinicians track growth rate precisely: [before age 4, a growth velocity under 6 cm per year is a red flag; between ages 4 and 8, under 5 cm per year; before puberty, under 4 cm per year.
](https://www. merckmanuals. com/professional/pediatrics/endocrine-disorders-in-children/growth-hormone-deficiency-in-children) These cutoffs help identify when the hormone axis might not be functioning as it should. Thyroid hormone matters too, as does cortisol: excess glucocorticoids (like those from chronic steroid medication) directly suppress chondrocyte proliferation and hypertrophy, which is one clear mechanism by which chronic illness or steroid treatment can stunt growth.
Growth plate closure is the endpoint. Over time, the plates lose height progressively and eventually fuse entirely through a process where cartilage is fully replaced by bone. Once fused, the bone has no mechanism left for longitudinal growth. This is why adults generally do not grow taller, and why questions about growing taller in adulthood have very different answers than questions about childhood growth. For adults, that is also why questions about growing taller after the growth plates fuse have very different answers than childhood growth growing taller in adulthood. This is why answering what makes a person grow taller depends on the status of the growth plates and the hormonal signals that drive them.
Genetics vs environment: what sets your height ceiling
Height is one of the most heritable traits we have. Twin studies consistently estimate heritability at around 80%, meaning most of the variation in height between people comes down to genes. Large genome-wide studies have now identified thousands of common genetic variants that each contribute tiny effects, and together common variants account for roughly 50% of the heritable contribution to height variation. The architecture is massively polygenic: no single gene runs the show. A useful clinical shortcut is midparental height, calculated by averaging both parents' heights (with a correction for sex), which gives a rough target range for a child's expected adult height.
That said, genetics sets a range, not a fixed number. Environmental inputs determine where within that range you actually land. A child with excellent genetic potential who is chronically undernourished or dealing with untreated illness may fall well short of their ceiling. Conversely, no amount of optimal nutrition or sleep will push someone meaningfully above their genetic ceiling. The distinction matters because it shapes realistic expectations: the goal of optimizing lifestyle factors is to reach your potential, not to exceed it.
What drives growth in childhood: nutrition is the biggest lever

Adequate calories are the baseline. A child who is not eating enough simply cannot sustain the cellular energy demands of continuous bone growth. Beyond total calories, specific nutrients have meaningful evidence behind them. Systematic reviews of nutrition interventions in children over age two find that protein, zinc, vitamin A, and multiple micronutrients together show significant positive effects on linear growth. Zinc in particular shows stronger benefits in populations with existing growth faltering or stunting, suggesting it matters most when there is a real deficiency to correct.
Vitamin D is worth addressing specifically because it gets a lot of attention. It is genuinely important for bone mineralization and skeletal health, and correcting severe deficiency matters. However, a 2024 meta-analysis found that vitamin D3 supplementation alone showed no significant improvement in height-for-age Z-scores in the included trials. The nuance here is that vitamin D is more reliably linked to bone density outcomes than to linear height gains. Calcium and iron, similarly, do not consistently show linear-growth benefits in the evidence base, though they are still essential for overall bone and blood health.
The practical takeaway: a varied, protein-rich, micronutrient-complete diet is the best nutritional strategy for supporting healthy growth in children. Targeted supplementation is most useful when a specific deficiency is identified, not as a general height-boosting measure. Oral nutritional supplementation can support catch-up growth in children with genuine undernutrition, but it does not push well-nourished children above their genetic potential.
Sleep and stress: recovery is not optional for growth
Growth hormone is not released in a steady trickle. It comes out in pulses, and the largest of those pulses happens during slow-wave (deep) sleep. This is well-established physiology: slow-wave sleep and GH release are tightly linked. Research on psychosocial dwarfism, a condition where severe emotional deprivation causes growth failure, makes the connection even clearer. Studies found that stage IV sleep deficits in these children were associated with reversible GH deficiency, and that when the children were placed in healthier environments, sleep normalized, GH secretion recovered, and growth velocity increased. That is a dramatic natural experiment showing how profoundly the sleep-stress-hormone axis affects real bone growth.
It is worth being precise about what the evidence does and does not say. One study found that acute sleep disruption in pubertal children did not consistently reduce pulsatile GH secretion, suggesting it is chronic patterns of poor or disrupted sleep rather than a single bad night that poses the real risk. Chronic stress is the bigger concern too: sustained high cortisol directly suppresses growth plate activity at the cellular level by downregulating GH receptor and IGF-1 signaling in chondrocytes. For growing children, consistent sleep, a stable home environment, and management of chronic stress are not soft lifestyle suggestions; they are physiologically relevant to how tall that child will grow.
Exercise and movement: what actually helps (and what does not)

Regular physical activity supports healthy bone development in children. High-impact, weight-bearing activities like jumping, running, and sports appear to stimulate skeletal adaptation and positive bone gain. A 24-week jumping protocol study in children with short stature was designed specifically to evaluate whether impact loading affects bone mineral density and linear growth, reflecting genuine scientific interest in whether activity patterns matter. The broad evidence suggests that appropriate physical activity supports a healthy growth environment, though it is not a direct override of genetic or hormonal limits.
For adults, the picture is completely different. No exercise, including stretching, yoga, or any targeted program, can reopen fused growth plates. The evidence on this is clear. One study measuring the effect of stretching on recorded height found a change of about 0.
28 cm, which is within the range of normal diurnal variation in stature (you are taller in the morning than at night due to spinal disc compression), not a true skeletal change. A biomechanical model also links spinal loading to measurable intervertebral disc height loss over hours, which helps explain why adults may appear slightly shorter later in the day [taller in the morning than at night due to spinal disc compression](https://pubmed. ncbi. nlm.
nih. gov/10451048/). Any product or program promising adults lasting height gains through exercise or stretching is not supported by good evidence. What exercise genuinely does for adults is improve posture and core strength, which can affect how tall you appear and how you carry yourself, but that is a very different claim from actually growing taller.
Puberty, growth spurts, and why timing changes everything
Puberty is the period of fastest height growth outside of infancy. Sex steroids, particularly estrogen and testosterone, supercharge the GH/IGF-1 axis and accelerate growth plate activity, producing the adolescent growth spurt. But the timing of that spurt varies considerably between individuals, and the timing has real consequences for height trajectory.
Boys, on average, go through their growth spurt about two years later than girls. This is why many girls are taller than their male classmates in early adolescence, and then the pattern reverses. Within each sex, early maturers tend to be taller than peers during early-to-mid adolescence, but because their growth plates fuse sooner, they often end up at a similar or even slightly shorter final adult height compared to late maturers who grow for longer.
If you are worried about what makes you grow shorter, it often comes down to factors like delayed puberty timing, poor nutrition, chronic stress, or conditions that interfere with growth plate activity shorter final adult height. A child who seems short at age 13 but has a late pubertal timing may simply be on a slower clock, not on a path to a shorter adult height.
This is called constitutional delay of growth and puberty, and it is a normal variant, not a disorder.
Peak height velocity, the moment of fastest growth during the spurt, does not line up neatly with a specific Tanner stage across all individuals. Some children grow fastest early in puberty, others later. Growth charts and serial measurements over time give a much clearer picture of where a child actually is in their trajectory than a single snapshot measurement.
Adult height: why you stop growing and what changes with age
Once growth plates fuse, long bones cannot lengthen further. This is a structural biological endpoint, not a limitation that can be overcome. Epiphyseal fusion happens progressively across different bones and is typically complete by the late teens in most females and early-to-mid twenties in most males, with individual variation.
What does change in adult height is spinal. The spine accounts for roughly a third of standing height, and it is susceptible to cumulative changes over decades. Intervertebral discs compress throughout the day under spinal loading (which is why most people are measurably shorter by evening), and over years, disc dehydration and thinning become permanent. Vertebral compression fractures, often driven by osteoporosis, can cause sudden measurable height loss, and stooped posture from muscle weakness or spinal deformity compounds the effect.
A 34-year longitudinal study found meaningful correlations between spinal deformity, degeneration, and height loss in older adults. Harvard Health and the Cleveland Clinic both point to these vertebral and disc changes as the primary mechanisms behind why adults lose height with age, estimating that people can lose one to three inches or more over a lifetime.
None of this means adults are helpless. Maintaining bone density through adequate calcium and vitamin D intake, resistance training, and impact exercise reduces the risk of compression fractures. Good posture and core strength preserve measured standing height. These are real, practical strategies, they just work by preventing height loss rather than adding new height. If you are asking whether it is possible to grow shorter, the key point is that growth plates can only shorten or change height through factors like posture changes or spinal disc compression, not by intentionally reversing bone lengthening is it possible to grow shorter.
Myths worth dropping right now
- Height pills and supplements: no product sold over the counter can stimulate growth plate activity in a normally functioning child or reopen plates in an adult. If a supplement contains anything that genuinely affects GH secretion at meaningful doses, it would be a regulated drug, not a supplement.
- Stretching for permanent height: the ~0.28 cm change measured in stretching studies is a transient measurement artifact, not bone elongation. Consistent stretching improves flexibility and posture but does not lengthen your skeleton.
- Special diets that make you taller: no specific food unlocks height beyond correcting an actual deficiency. Protein, zinc, and sufficient calories matter in the context of overall adequate nutrition, not as magic inputs.
- Adults can grow taller with the right program: this is false if growth plates are fused. Any apparent 'gain' reflects posture improvement or measurement variability, not skeletal growth.
- Late puberty always means shorter adult height: not necessarily. Late maturers often have longer growth windows and can reach similar or taller final heights than early maturers.
How to assess growth status and when to get help
For children and teenagers, the most useful tool is a growth chart plotted over time. A single height measurement tells you very little; growth velocity (how fast a child is growing over months) is far more informative. Most pediatricians track this at well-child visits. Red flags that warrant further evaluation include growth velocity below the clinical cutoffs mentioned earlier, a child crossing percentile lines downward over time, a height significantly below the midparental target range, or any signs of delayed or early puberty.
If a pediatrician suspects a hormonal or genetic cause, the next step is typically a referral to a pediatric endocrinologist. Evaluation may include IGF-1 and GH testing, thyroid function tests, bone age X-ray (to compare skeletal maturity to chronological age), and sometimes genetic testing. Many cases of short stature turn out to be familial short stature or constitutional delay, both normal variants, but ruling out treatable conditions early matters because some interventions (like GH therapy) are time-sensitive and only effective before growth plates close.
Practical habits that genuinely support healthy growth
| Factor | What the evidence supports | Realistic expectation |
|---|---|---|
| Adequate calories and protein | Essential for sustaining growth plate activity and cellular energy demands | Prevents growth faltering; does not push above genetic ceiling |
| Zinc and micronutrients | Zinc shows significant positive effects on linear growth, especially in deficient populations | Most relevant when correcting a true deficiency |
| Vitamin D | Important for bone mineralization and density; limited evidence for direct height gains | Supports skeletal health; correct deficiency but don't expect height gains |
| Consistent, quality sleep | Deep sleep drives GH pulse release; chronic disruption linked to reversible growth problems | Protects growth trajectory; does not add height above potential |
| Physical activity (impact/weight-bearing) | Supports bone gain and healthy development in children | Growth-supportive environment; not a height override |
| Low chronic stress | Sustained cortisol suppresses growth plate activity directly | Managing stress preserves growth velocity |
| Posture and core strength (adults) | Affects measured standing height and long-term spinal health | Prevents height loss; does not add skeletal height |
The bottom line is that height growth is a tightly regulated biological process driven by growth plate biology and the endocrine system, shaped heavily by genetics, and modifiable mainly through the basics: eat well, sleep consistently, move regularly, and address medical issues early. There is no shortcut that bypasses the underlying biology, but there is also real room to optimize within your genetic range, especially during the years when growth plates are still open. If you are asking can you grow smaller, it is usually about reducing height through posture changes or when growth plates are still open, but the details depend on age and underlying health.
FAQ
How can I tell if a child’s height issue is about growth speed or just a normal family pattern?
Look at growth velocity over time (usually over 6 to 12 months) and compare it with the child’s midparental height target. A child can be short but growing normally if they follow a steady curve, while a child who drops percentiles downward or has slowed velocity despite adequate nutrition should be evaluated sooner.
Does measuring height at home at different times of day make results unreliable?
Yes. Standing height varies with daily spinal loading, so morning measurements are typically higher than evening. For tracking growth, use consistent methods (same time of day, same measurement technique, barefoot, similar posture) and rely on trends rather than single readings.
Can a bone age X-ray tell whether growth plates are already too close to closing?
It helps estimate skeletal maturity by comparing the growth plate and other bone-development markers to chronological age. This is especially useful when puberty timing is unclear, because some conditions or constitutional delay can make a child’s timeline look different even if growth velocity seems borderline.
Is it ever possible to “reopen” growth plates with supplements, stretching, or hormone pills?
No for typical adulthood. Once epiphyseal fusion occurs, longitudinal growth cannot resume, and stretching or supplements cannot reverse that. For children, certain hormone treatments (for example, prescribed growth hormone in specific deficiencies) can help, but only when a clinician confirms an underlying treatable cause.
If vitamin D doesn’t improve height-for-age in trials, should my child still get tested or supplemented?
If there is risk of deficiency or signs of bone health problems, testing can still be useful, and severe deficiency should be corrected for skeletal health. The key distinction is that correcting vitamin D alone is not a reliable height-boosting strategy when the main goal is linear growth.
What role does puberty timing play in whether a teen ends up taller or shorter?
Timing affects how long growth plates stay active and when the adolescent growth spurt occurs. Early maturers may look taller at first, then fuse sooner, sometimes leading to similar or slightly shorter adult height compared with late maturers who grow for longer. Tracking growth rate across puberty is more informative than a single Tanner stage label.
Are growth charts enough, or can two children on the same percentile still have different risk?
Yes. Percentiles summarize where height falls at one point in time, but they do not capture how fast height is increasing. Serial measurements that show stable velocity suggest lower concern, while decreasing percentiles or persistently slow velocity increases the likelihood of an underlying issue.
What are common reasons a child’s growth velocity might drop besides hormones?
Chronic undernutrition, chronic inflammatory illness, celiac disease, uncontrolled asthma requiring long-term steroid treatment, and significant psychosocial stress can all reduce growth plate activity through reduced energy availability or higher cortisol effects. Persistent symptoms or weight changes alongside slowed growth should raise suspicion.
If a child is short, when should parents ask about a pediatric endocrinology referral?
Consider referral when growth velocity is below the clinical cutoffs, when the child crosses downward through major percentile lines, when height is far below the midparental target, or when puberty appears significantly delayed or advanced. Early evaluation matters because some interventions are time-sensitive before growth plates close.
Do height-increasing foods or supplements work as a general strategy for healthy kids?
In a well-nourished child, broad supplementation usually does not override genetic ceiling or open closed growth plates. The most reliable approach is correcting specific deficiencies when identified, ensuring adequate total calories and protein, and addressing medical issues that impair growth.
Can posture training or braces increase measured height for adults?
They can sometimes improve measured standing height by reducing stooped posture or spinal curvature, but they do not lengthen fused bones. The change is typically about appearance and alignment rather than true skeletal growth, so expectations should be set accordingly.
Next Article
How Does the Body Grow Taller? Growth Science and What Helps
Learn how bone growth plates lengthen the body, how hormones and sleep affect height, and what helps by age.
