Grapes won't make you grow taller. No single food will. Does orange juice help you grow taller? The answer is similar: it cannot override growth-plate biology, and extra juice does not translate into extra height. But grapes are genuinely nutritious, and the nutrients they contain do play supporting roles in healthy bone development and overall growth when you're still in a phase of life where growth is biologically possible. The honest answer is that grapes can be a useful part of a growth-supporting diet, especially for kids and teenagers whose growth plates are still open, but they don't have any special height-boosting power that sets them apart from other fruits or vegetables.
Do Grapes Help You Grow Taller? What the Evidence Says

Marcus Reeves
9 Jun 2026

What 'grapes for height' claims usually mean

Most claims connecting grapes to height growth point to a few specific compounds. Resveratrol is the big one, a polyphenol found in grape skins that gets a lot of attention for its antioxidant and anti-inflammatory properties. You'll also see mentions of vitamin C (grapes have modest amounts), vitamin K, and certain B vitamins. The idea is usually that these compounds support bone health, which then translates into taller stature.
The leap from 'supports bone health' to 'makes you taller' is where things fall apart. Bone health and linear growth are related but not the same thing. Strong, dense bones are great, but they don't mean your skeleton will add length. Height increase requires active growth at the growth plates, the cartilaginous zones near the ends of your long bones, which is a hormonally driven process with a hard biological endpoint. A grape, or any food for that matter, can't switch that process on or extend it beyond what your genetics and developmental timing allow.
What the evidence actually says about grapes, their nutrients, and growth
Let's look at the specific nutrients tied to these claims and what the research actually shows, because it's more nuanced than a simple yes or no.
Resveratrol

Resveratrol is probably the most-cited reason people link grapes to bone and height benefits. But a systematic review and meta-analysis of randomized controlled trials found that resveratrol supplementation did not produce significant changes in bone serum markers, including alkaline phosphatase and osteocalcin, markers that reflect bone formation activity. That's supplemental resveratrol in concentrated doses, not the small amounts you'd get from eating a handful of grapes. The evidence just isn't there.
Vitamin C
Grapes contain some vitamin C, which is involved in collagen synthesis, a protein that gives bones and cartilage their structural integrity. Severe vitamin C deficiency (scurvy) does cause bone and connective tissue problems. But according to the Linus Pauling Institute, vitamin C status has not been consistently associated with bone health measures in observational studies among people who aren't deficient. Getting enough is important; getting extra from grapes won't build extra height.
Vitamin K and other micronutrients
Vitamin K plays a role in bone metabolism, and there's reasonable evidence that adequate intake supports bone health generally. Grapes contain small amounts of vitamin K, particularly vitamin K1. But again, the framing here is deficiency prevention and general skeletal health, not height gain. The research on vitamin K and bone is not about growth-plate activity or linear growth velocity. A review on vitamin K summarizes evidence that vitamin K plays a role in bone and discusses vitamin K sufficiency and bone health framed around general bone health rather than growth-plate or height-gain outcomes not about growth-plate activity or linear growth..
Kids, teens, and adults: the evidence looks different depending on your age
For children and pre-teens whose growth plates are still wide open, nutrition absolutely matters for reaching full growth potential. Deficiencies in key nutrients like calcium, vitamin D, zinc, and protein can impair growth. The WHO framework on childhood stunting makes it clear that linear growth outcomes depend on multiple interacting factors, not any single food. Getting adequate overall nutrition, including fruit like grapes, is beneficial, but no specific food is the lever that unlocks height.
For teenagers in the middle of a growth spurt, the same principle applies with even more intensity because calorie and nutrient demands are higher. The growth spurt is hormonally driven (more on that below), and good nutrition creates the biological conditions for that process to proceed well. Grapes fit in as part of a varied diet but hold no special status.
For adults whose growth plates have fused, the answer is simply that height increase is not happening through nutrition or any other non-surgical means. Diet still matters enormously for health, but it won't add centimeters to your frame.
How height actually increases: growth plates, hormones, and genetics
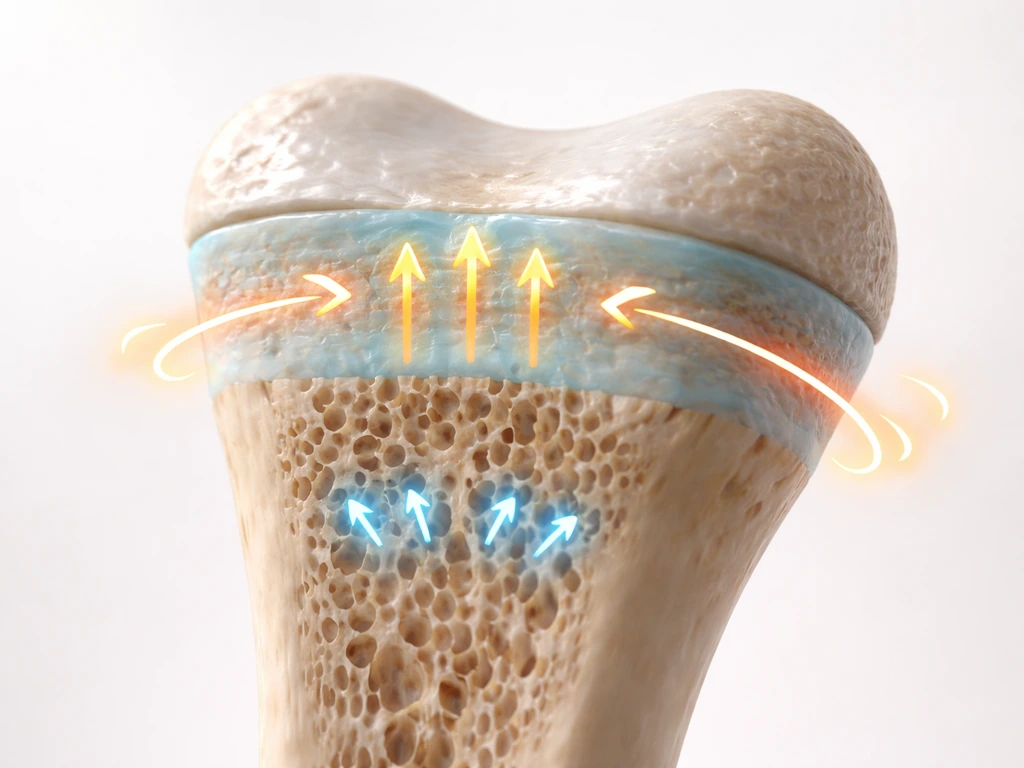
To understand why diet can't be the primary driver of height, you need a basic picture of how height increase works. Long bones grow in length at regions called epiphyseal growth plates, layers of cartilage located near the ends of bones like the femur and tibia. New cartilage cells are produced, then progressively replaced by bone tissue, extending the bone's length over time.
This process is controlled largely by hormones. Growth hormone (GH) is secreted by the pituitary gland, and it stimulates the liver to produce IGF-1 (insulin-like growth factor 1), which acts directly on growth plates. Sleep is critical here: GH secretion during sleep is primarily dependent on growth hormone-releasing hormone pulses, meaning deep, consistent sleep isn't optional if you want normal growth. During puberty, rising estradiol levels in girls, and estradiol produced from testosterone in boys, directly stimulate GH release, which is why the pubertal growth spurt is so pronounced.
The endpoint of growth is fusion of the growth plates. Once those plates close, bone mineral density can still change, but bone length cannot. An X-ray to assess bone age, measuring the maturity of the bony growth plates, can estimate how much time a person has left to grow. This is a standard clinical tool used by endocrinologists precisely because growth is a biological timetable, not an open-ended process that better nutrition can extend indefinitely. Genetics sets the ceiling; nutrition and lifestyle determine how close you get to that ceiling.
Nutrition that actually supports growth (not just grapes)
If you want to give your body, or your child's body, the best nutritional conditions for reaching full height potential, the focus should be on overall dietary quality and making sure key growth-relevant nutrients are covered. Here's where the evidence is clearest:
| Nutrient | Why it matters for growth | Good food sources |
|---|---|---|
| Protein | Provides amino acids needed for tissue synthesis, including bone matrix and IGF-1 production | Meat, poultry, fish, eggs, dairy, legumes |
| Calcium | Essential for bone mineralization; deficiency can cause rickets and impaired skeletal development in children | Dairy, fortified plant milks, leafy greens, sardines |
| Vitamin D | Required for calcium absorption; deficiency in children causes rickets and stunted skeletal development | Fatty fish, fortified milk, sunlight exposure, supplements if needed |
| Zinc | Impaired growth in children can be a sign of zinc deficiency; zinc is involved in cell division and protein synthesis | Meat, shellfish, legumes, seeds, dairy |
| Vitamin A | Supports growth-related cell functions; deficiency is linked to adverse developmental outcomes | Liver, dairy, eggs, orange/yellow vegetables, leafy greens |
| Overall calories | Chronic caloric insufficiency is one of the most direct causes of growth faltering | Varied, balanced diet with sufficient energy for age and activity level |
Notice that grapes don't appear on that list as a standout source of any of these critical nutrients. If you're wondering whether almonds can do the same thing, the answer is still about overall nutrition and meeting nutrient needs, not a guaranteed height boost do almonds help you grow taller. They do contain modest amounts of vitamin C, vitamin K, and some B vitamins, and they're a good source of antioxidants and hydration. Including them in a diet is smart. Relying on them as a height strategy is not.
If you're wondering about other fruits and their roles in growth, similar logic applies across the board. Whether it's bananas, apples, kiwis, or oranges, the nutritional contribution is real and valuable as part of a complete diet, but no fruit directly triggers taller stature on its own. If you're trying to grow taller, it's more about hitting the right growth-supporting nutrients overall than picking one specific fruit.
Sleep, exercise, and the lifestyle factors that genuinely move the needle

Sleep is probably the most underrated growth factor
Because GH secretion is so tightly tied to sleep, getting enough high-quality sleep during childhood and adolescence is one of the most concrete things you can do to support normal growth. The American Academy of Pediatrics recommends 9 to 12 hours per night for children aged 6 to 12, and 8 to 10 hours for adolescents aged 13 to 18. These aren't soft suggestions; sleep deprivation chronically disrupts GH release. Prioritizing consistent bedtimes and eliminating screens before bed is practical, evidence-aligned advice.
Exercise and bone loading
Regular physical activity, especially weight-bearing and impact activity like running, jumping, and resistance training, supports bone mineral accrual in children and adolescents. That's a well-documented effect. What it does not do is directly increase linear growth rate or ultimate height in people who are otherwise healthy and well-nourished. An NCBI review of the literature makes it clear that regular physical activity has no established effect on linear growth rate or final adult height.
That said, the AAP has confirmed that well-designed resistance training programs are safe for youth and don't negatively affect growth plates. So there's no reason to avoid weights out of fear of 'stunting growth,' which is a myth. The CDC recommends that children and adolescents get muscle- and bone-strengthening activities like running, jumping, and resistance exercises as part of their weekly physical activity. These habits build health broadly, which supports normal development.
Other lifestyle factors worth mentioning
- Avoiding growth inhibitors: chronic illness, severe undernutrition, and prolonged high-dose corticosteroid use (for conditions like asthma or autoimmune disease) can impair growth. If a child is on long-term medications, this is worth discussing with a doctor.
- Managing stress and psychosocial environment: the WHO framework on stunting explicitly includes inadequate psychosocial stimulation as a factor affecting linear growth outcomes, not just nutrition.
- Maintaining a healthy body weight: both underweight (caloric deficit) and severe obesity can affect growth hormones and pubertal timing, which in turn affect height trajectory.
- Posture: while not the same as actual height increase, improving posture can help people stand at their full measured height rather than appearing shorter due to habitual slouching.
Realistic expectations and knowing when to see a doctor
If you're a parent monitoring your child's growth, the key signal to watch for isn't a specific height number but a pattern. Dropping progressively across growth curve percentiles over time, say from the 25th to the 5th percentile, is a more meaningful concern than simply being shorter than peers. Children's Mercy notes that height velocity that is slow for age and gender warrants evaluation, while a child who is short but growing at a normal rate and has no other suspicious features very rarely has a true growth problem.
The Endocrine Society describes that medical evaluation of growth concerns focuses on identifying treatable medical causes versus normal variation, such as familial short stature or constitutional delay of growth and puberty. Bone age X-rays are commonly used to estimate remaining growth potential. If there is a treatable underlying cause, like growth hormone deficiency, hypothyroidism, or celiac disease affecting nutrient absorption, addressing that condition is the intervention that matters, not adjusting fruit intake.
For teenagers worried about their own height: if your growth plates are still open, optimizing sleep, hitting nutritional targets, staying active, and managing your overall health is the genuine playbook. If you're a young adult who has finished puberty and your growth plates have closed, your height is set. Good nutrition and exercise still matter enormously for your health, longevity, and how you feel, just not for adding inches.
If there are real concerns about growth, whether delayed puberty, falling off the growth curve, or suspected endocrine issues, a pediatrician or pediatric endocrinologist is the right resource. A referral threshold that's commonly used is height below the 3rd percentile with a slow height velocity, though any persistent concern warrants a conversation with a clinician. Eating more grapes is not a substitute for that conversation. Walnuts are often discussed for nutrition, but they do not change growth-plate biology, so they cannot guarantee helping you grow taller walnuts help you grow taller.
FAQ
If I eat more grapes, can they make a noticeable difference in height for my child or teen?
Usually no. Grapes can support overall nutrition, but height gains require active growth at the growth plates. A noticeable difference typically does not come from one food, especially when the child’s total calories, protein, calcium, and vitamin D are already adequate.
What nutrient gaps would actually limit growth, and how do I know if grapes might help?
Growth can be limited by deficiencies in calories, protein, calcium, vitamin D, zinc, and sometimes iron, plus conditions that reduce absorption. Grapes are not a major source of the key nutrients that clinicians look for, so grapes help only indirectly by improving diet quality rather than correcting a specific deficiency.
Do grape products like juice or supplements work better than whole grapes for height?
Not in a height-specific way. Juice has less fiber and can add sugar without delivering extra growth-critical nutrients, and concentrated supplements (for example, high-dose resveratrol) have not shown evidence of improving bone formation markers. Whole-food approaches are generally the safer, more practical option.
Are red grapes or grape seed extracts more likely to help with height than regular grapes?
There is no good evidence that either changes linear growth. Grape seed extracts and grape-derived compounds may have antioxidant activity, but they do not meaningfully turn on growth-plate growth or extend the growth timeline.
Can grapes help if my child is short but otherwise healthy and growing steadily?
If growth velocity is normal and there are no concerning symptoms, the most useful step is usually to ensure overall nutrition and sleep rather than increase grapes. A steady growth pattern often reflects normal variation, and clinicians prioritize growth rate and medical history over single-food changes.
What signs suggest we should check with a pediatric endocrinologist rather than adjust the diet?
Consider evaluation if height is very low for age (often below the 3rd percentile) and growth velocity is slow, if there is a clear downward crossing of percentiles over time, or if puberty timing is markedly delayed or absent. Persistent fatigue, weight loss, GI symptoms, or frequent illnesses can also warrant medical assessment.
Does exercise plus grapes work together to increase height more than exercise alone?
Exercise supports bone strength and healthy development, but it does not directly increase linear growth rate in otherwise healthy youth. Grapes can be part of a well-rounded diet that helps meet nutrient needs, but they are not an additive “height boost” on top of activity.
Can sleep, protein, and vitamin D be the real reason people think grapes helped them grow taller?
Yes. Many height improvements that appear “food-related” happen alongside other growth drivers like adequate sleep, enough total calories, higher protein intake, and improved overall health. Grapes may coincide with better habits, which can create the impression they caused the change.
Is there any situation where grapes might indirectly support growth outcomes?
They can help if they improve adherence to a balanced diet, especially when they replace less nutritious choices. They may also contribute small amounts of vitamins and antioxidants that support general bone and tissue health, which matters most during the years when growth is still possible.
After growth plates close, do grapes help with bone density even if they cannot increase height?
Yes, grapes can still support general bone health through their nutrient content and antioxidants, and a healthy diet is beneficial for long-term skeletal health. However, bone density changes do not translate into added bone length or increased height once growth plates have fused.
Next Article
Do Almonds Help You Grow Taller? What Science Says
Science says almonds rarely increase height; genetics and growth plates matter most. Use almonds to support nutrition sa
