Whether you'll grow as tall as your dad depends heavily on genetics, but it's not a simple copy-paste from father to child. Height is about 60–80% heritable, and your dad is only one of two genetic contributors. Most people end up somewhere in a range predicted by both parents' heights combined, and about 95% of kids land within roughly 4 inches (10 cm) above or below that family midpoint. So matching your dad's exact height is possible, exceeding it is possible, and falling short is also possible. The good news is that the 20–40% of height variation that isn't genetic is something you can actually do something about.
Will I Grow as Tall as My Dad? Genetics and Growth Factors

Marcus Reeves
29 May 2026
How accurate is "I'll match my dad's height"?
The intuition that you'll end up close to your dad's height isn't wrong, but it's too simple. Height is a polygenic trait, meaning hundreds or even thousands of genetic variants each contribute a tiny piece of your final stature. You don't inherit a single "tall gene" from your dad. You inherit a shuffled mix of genetic variants from both parents, and the combination you get is somewhat unpredictable at the individual level.
There's also a well-documented phenomenon called regression to the mean. If your dad is unusually tall, you're statistically likely to be shorter than him. If he's unusually short, you're likely to be taller than him. Both of your parents' heights pull you toward the population average to some degree. This doesn't mean you can't match a very tall dad, but the odds shift depending on where your parents sit relative to average height.
The practical takeaway: your dad's height is one important data point, but it's not a ceiling or a guarantee. Your mom's height matters just as much, and the full genetic mosaic you inherited from both sides determines your ceiling more than either parent's height alone.
Using your parents' heights to estimate your height range

The mid-parental height (MPH) method is the standard tool clinicians use to estimate a child's adult height potential. It's not perfect, but it gives you a useful reference range to work with. The calculation adjusts for sex and averages both parents' heights.
- For boys: add your dad's height (in inches) and your mom's height (in inches), add 5 inches, then divide by 2.
- For girls: add both parents' heights (in inches), subtract 5 inches, then divide by 2.
- That result is your mid-parental target height. Your predicted adult height range is that number plus or minus about 4 inches (10 cm).
Example: if your dad is 5'10" (70 inches) and your mom is 5'5" (65 inches), a boy's mid-parental height would be (70 + 65 + 5) / 2 = 70 inches, or 5'10". The predicted range is roughly 5'6" to 6'2". That's a wide window, and it's intentional. About 95% of kids fall within that 8-inch band. Notice that in this example the boy could realistically match or even exceed his dad while also potentially ending up shorter.
This formula is a starting point, not a verdict. More accurate predictions come from combining it with a child's current growth trajectory on standardized growth charts and, most precisely, a bone age X-ray. More on those below.
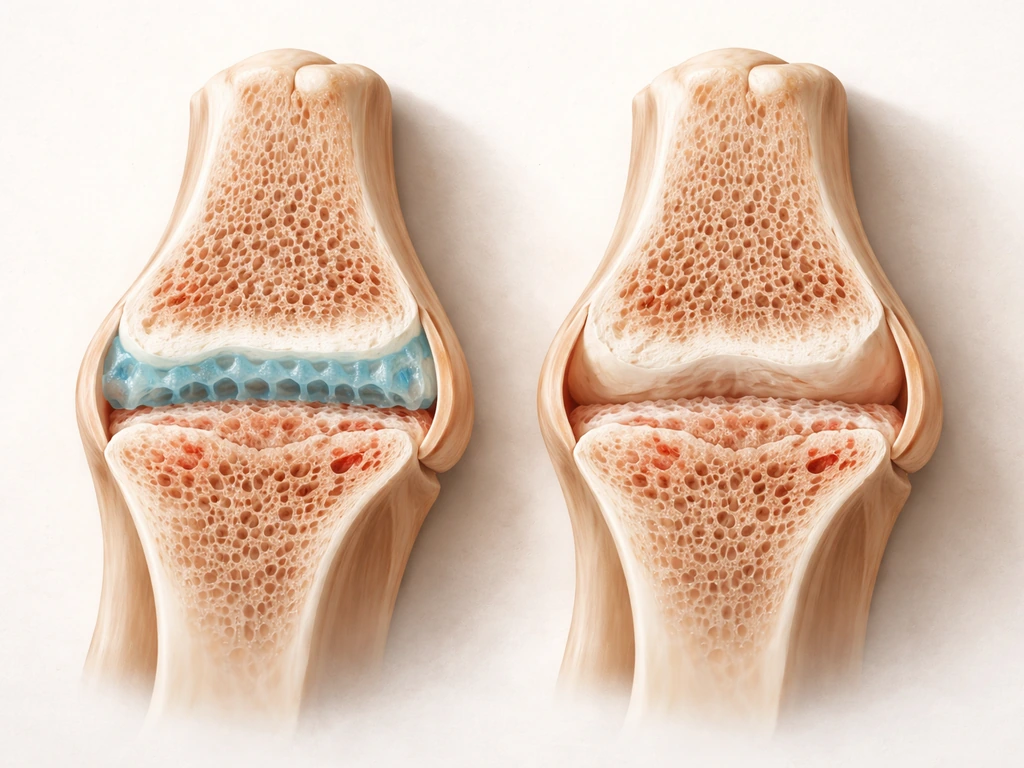
Where growth actually happens: puberty, growth spurts, and growth plates
Your long bones grow at specialized areas near the ends called growth plates (epiphyseal plates). While these plates remain open, you can still gain height. Once they close (fuse), linear growth stops completely. This is why timing matters so much.
Puberty timing and the growth spurt
For boys, the main growth spurt typically happens between ages 12 and 16, with peak velocity usually around ages 13–14. During the peak year, boys can gain more than 10 cm (about 4 inches). After puberty wraps up, most teens gain only about 1–2 more inches before growth plates fully close. Girls generally start their growth spurt earlier, around age 11.5 on average, and typically grow only about 2–3 inches after their first period.
Puberty onset that's earlier or later than average shifts this whole timeline. Precocious puberty (before age 8 in girls, before age 9 in boys) can actually limit final height because growth plates close earlier. Delayed puberty (no signs by age 13 in girls or 14 in boys) often means a later but still substantial growth spurt. You can also watch for signs that puberty is delayed, such as no growth spurt or other puberty changes by the expected ages Delayed puberty. If you're a late bloomer, you may still have significant growing ahead of you even when peers seem to have stopped.
One practical implication: if you're mid-puberty right now, you're likely in or approaching your best window to support growth. If you've already finished puberty, the growth plates are likely closing or closed, and the honest reality is that meaningful height gain from here is limited regardless of what you do.
Lifestyle factors you can actually control
Genetics sets the ceiling, but lifestyle can meaningfully affect how close you get to it. If you stop vaping, that can be part of making your lifestyle healthier during the years your body is still growing lifestyle can meaningfully affect. The research is clearest on correcting deficiencies rather than boosting height above your genetic potential, but during active growth those deficiencies matter a lot.
Nutrition

Adequate total calories and protein are the foundation. Growing bones and tissues require raw material, and chronic undereating is one of the clearest ways to fall short of your genetic height potential. Beyond calories, specific micronutrients matter most: calcium and vitamin D are critical for bone mineralization, zinc deficiency has been directly linked to impaired linear growth (with supplementation showing small but measurable improvements in some studies), and iron deficiency is another flag since it's associated with stunted growth and is a condition clinicians screen for during short stature evaluations. A well-rounded whole food diet covering these bases is more effective and safer than throwing individual supplements at the problem.
Sleep
Growth hormone is released primarily during deep, slow-wave sleep, which is why sleep isn't just good for energy but is a direct input into the growth process. The American Academy of Sleep Medicine, endorsed by the AAP, recommends teenagers get 8–10 hours per night consistently. Chronically sleeping 5–6 hours during peak growth years isn't neutral. It compresses the window for growth hormone secretion. This is especially relevant in early adolescence when the growth spurt is most active.
Exercise and physical activity
Regular physical activity supports healthy bone density and overall development, but a few myths need clearing up. Stretching does not make you taller by elongating bones. Flexibility work improves posture and range of motion, not growth plate outcomes. Weight-bearing exercise and sports are positive for bone strength, but growth plate injuries (which are a real risk during rapid growth phases) can actually impair growth if severe. If you're in an intense training program during a growth spurt, protecting your joints and growth plates matters more than pushing maximum loads.
Health factors that can quietly limit your height
Sometimes the gap between genetic potential and actual height is caused by an underlying health issue rather than lifestyle. These are worth knowing about because many are treatable, and catching them early makes a real difference.
- Celiac disease and inflammatory bowel disease: both impair nutrient absorption in the gut, which can directly reduce growth even when food intake looks adequate.
- Kidney disease: chronic kidney problems affect bone metabolism and can suppress growth hormone pathways.
- Hypothyroidism: thyroid hormone plays a direct role in regulating growth, and untreated low thyroid function is a classic cause of slowed growth in children.
- Anemia (iron deficiency): consistently flagged in short stature evaluations as a correctable contributor to poor growth.
- Growth hormone deficiency: a less common but important cause of falling significantly below the mid-parental height range.
- Precocious puberty: early puberty can mean shorter adult height because growth plates close sooner than they should.
The Endocrine Society specifically lists anemia, kidney issues, celiac sensitivity, hypothyroidism, and hormone abnormalities as standard things to screen for when a child isn't growing as expected. If you're noticeably below your predicted height range and your lifestyle factors check out, a health issue may be the missing piece.
Can you actually grow taller than your dad? What shifts the odds
Yes, you can exceed your dad's height, and it's more likely in specific scenarios. Here's what moves the odds in your favor:
| Factor | How it affects your odds of exceeding dad's height |
|---|---|
| Your mom is taller than your dad | The mid-parental calculation pulls your predicted range above dad's height, making it statistically more likely you'll pass him |
| Your dad is significantly above the population average | Regression to the mean works against matching him; you're statistically likely to end up closer to average than he is |
| Your dad is shorter than average | Regression to the mean works in your favor; your predicted height may actually be above his |
| You're still in early-to-mid puberty | The growth window is still open; optimizing nutrition, sleep, and health now has the most impact |
| You correct a nutritional deficiency | If your growth has been subtly limited by zinc, iron, or vitamin D deficiency, correcting it can unlock progress toward your genetic ceiling |
| You treat an underlying health issue | Conditions like celiac disease or hypothyroidism, when treated, can restore normal growth trajectory |
| You're a late developer | A later puberty timeline means more total growth time; late bloomers often end up taller than early-blooming peers expected |
What won't move the needle: no supplement, stretching routine, or exercise program will push you above your genetic ceiling. The ceiling is real. What these factors control is whether you reach that ceiling or fall short of it due to preventable causes.
How to check your actual growth potential right now
You don't have to guess. There are practical tools that give you a much clearer picture of where you stand and how much growth is likely left. If you want the most direct way to estimate how much growing time you may still have, ask about a bone age X-ray.
Step 1: Gather your data

- Your current age and height (measured accurately, standing straight against a wall in the morning when you're tallest)
- Both parents' measured heights (self-reported heights are often off by 1–2 inches; get actual measurements if possible)
- Any prior height measurements with dates (your pediatric growth chart if you have one)
- Your current puberty stage (have you started puberty, are you mid-way, or has it wrapped up?)
- Any known health conditions or symptoms like fatigue, poor appetite, or GI issues
Step 2: Plot yourself on a growth chart
CDC and WHO growth charts show where your current height falls relative to peers your age. More importantly, your growth trajectory over time (called growth velocity) tells a clinician a lot. If you've been consistently tracking along the 50th percentile and suddenly drop to the 25th, that's a red flag worth investigating. Growing less than 4 cm per year is a threshold that often triggers a referral to a specialist.
Step 3: Consider a bone age X-ray
The most accurate way to assess remaining height potential is a bone age X-ray of the left hand and wrist. It shows the maturity of your growth plates and how much growth time you realistically have left. A child with a bone age younger than their chronological age has more growth potential remaining. This is a routine, low-dose X-ray done in a pediatrician's or endocrinologist's office, and it's considered the most reliable method available for height prediction.
When to see a doctor
You should talk to a pediatrician or pediatric endocrinologist if: your height is significantly below your mid-parental target range (more than 4 inches below the calculated midpoint), your growth velocity has dropped or stalled, you haven't started puberty by age 14 (boys) or 13 (girls), or you have any of the chronic health symptoms listed earlier. Early evaluation opens up treatment options that simply aren't available once growth plates close. This connects to a broader question of what's truly still possible at your stage of development, which is worth exploring alongside understanding the signs that growth may be slowing or stopping.
Your practical next steps
If you're still growing, the path forward is straightforward. Calculate your mid-parental height range using both parents' measured heights. Compare your current height and growth trend to that range on a growth chart. Make sure the basics are covered: consistent 8–10 hours of sleep, adequate protein and calories, and no obvious nutritional gaps. If anything looks off, whether your height is tracking well below the mid-parental range, your growth seems to have slowed, or you have any health symptoms, get a pediatric evaluation sooner rather than later. A bone age X-ray can give you concrete, personalized data that no online calculator can match.
If puberty has already finished, the honest answer is that growth plate-based height gain is essentially done. At that point, posture, core strength, and spinal health are the levers that affect how tall you stand and carry yourself, not biological height. Accepting that distinction is more useful than chasing interventions that can't deliver on their promises.
FAQ
If my dad is unusually tall, does that mean I will almost definitely be close to his height?
You can still end up taller or shorter than your dad because your genetic mix comes from both parents. The simplest check is to use both parents’ measured heights (mid-parental height) and then see if your current height and growth velocity match that expected pattern.
Is there a quick way to estimate my adult height without a bone age X-ray?
Using your dad’s height alone is incomplete, especially if one parent is near average but the other is not. A better “sanity check” is comparing you to the mid-parental height range and then confirming with your growth chart trend over at least 6 to 12 months.
What should I do if my height is already below my mid-parental target range?
Mid-parental height range is a population estimate, not a personalized promise. If your growth velocity has slowed, dropped percentiles, or you are far below the range for your age, that signals you may have treatable factors rather than just “normal genetics.”
Can I catch up to my dad’s height if I’m behind right now?
Yes, but it depends on whether your growth plates are still open and whether the reason you are behind is correctable. If puberty is late and growth plates are less mature, there may be meaningful catch-up time, but only a clinician can judge this reliably with growth history and (often) bone age.
Does improving sleep actually change height, or is it too late once puberty starts?
Sleep matters most during active growth windows, but it is still relevant whenever you are a teenager growing. A practical detail is to aim for consistent bedtime and wake time, because irregular schedules can reduce the reliable deep-sleep window your body uses for growth hormone release.
Can stretching make me taller even if my growth plates are open?
Stretching and posture work are great for movement and appearance, but they do not reopen fused growth plates. If you want to focus on what helps while plates are open, prioritize adequate calories and protein, micronutrients (especially calcium and vitamin D), and safe weight-bearing activity.
What supplements should I take to maximize my chances of growing?
One common mistake is taking random supplements instead of fixing specific deficiencies. If you suspect low iron, vitamin D, or zinc, the safer next step is asking your pediatrician about targeted screening, since too much of some supplements can be harmful or mask other issues.
When should I stop waiting and ask a doctor about my growth?
The right “next step” varies by age and puberty stage. If you have not started puberty by the usual ages (boys by 14, girls by 13), or you have stalled growth velocity, that is typically a stronger reason for early evaluation than trying to adjust diet or training first.
If my dad is short, does that mean I cannot reach average height?
Even if your dad is short, you may still reach average or even above average depending on your mom’s height, your puberty timing, and whether your growth plate maturity is delayed. Regression to the mean can make “matching dad” less likely, but it does not determine your outcome by itself.
Can sports injuries permanently affect my ability to grow?
Yes. Severe or repeated growth-plate injuries during periods of rapid growth can impair linear growth if they are significant. If you play intense sports, focus on technique, adequate recovery, and get evaluated promptly after any injury that causes persistent pain or reduced function.
After puberty, can I still gain a bit of height through training or posture?
If you are finished with puberty and plates are fused, you generally cannot add true height biologically. You can still improve measured height in some cases by optimizing posture, strengthening the core, and addressing spinal issues, but those changes do not increase growth plate length.
Why do height prediction apps get it so wrong compared with doctors?
Online calculators often use only a simplified genetic estimate and ignore your growth velocity, puberty status, and skeletal maturity. The most informative approach is tracking your growth trend on standard charts and, when needed, using bone age to estimate remaining growth time.
Citations
Adult height is a highly heritable trait; studies estimate narrow-sense heritability for adult height at ~80% (i.e., a large fraction of population variation is attributable to genetic variation).
https://pmc.ncbi.nlm.nih.gov/articles/PMC4250049/
Large reviews of height genetics commonly summarize that narrow-sense heritability for adult height is ~60–80% (depending on the dataset/method), and height is polygenic (many genetic variants contribute).
https://pmc.ncbi.nlm.nih.gov/articles/PMC7263788/
Genome-wide association research suggests adult height variation is strongly influenced by common polygenic variation, consistent with polygenic inheritance rather than any single “height gene.”
https://pmc.ncbi.nlm.nih.gov/articles/PMC2681221/
Clinical guidance and patient resources emphasize that matching a parent’s exact height is not precise; adult height prediction uses a statistical range and accounts for population-level variation rather than a deterministic “equals dad” outcome.
https://eqipp.aap.org/courses/growth2/mn/clinical-guide/popups/mid-parental-height
Regression to the mean is expected in height inheritance: children tend to fall closer to the population average than extreme parental heights would suggest.
https://en.wikipedia.org/wiki/Regression_toward_the_mean
AAP’s mid-parental height estimate uses a target height range of “mid-parental height ± 10.2 cm.”
https://eqipp.aap.org/courses/growth2/mn/clinical-guide/popups/mid-parental-height
Using that mid-parental approach, “95% of children” have a predicted adult height within about 4 inches (≈10 cm) above or below the calculation.
https://eqipp.aap.org/courses/growth2/mn/clinical-guide/popups/mid-parental-height
HealthyChildren.org describes the common mid-parental method as: add parents’ measured heights and divide by 2 (with the midpoint used as the basis for prediction), and it also notes clinicians use growth charts to refine the estimate over time.
https://www.healthychildren.org/English/health-issues/conditions/Glands-Growth-Disorders/Pages/Predicting-a-Childs-Adult-Height.aspx?form=HealthyChildren
AAFP summarizes classic midparental height calculations that adjust for sex by using a ~5-inch (≈13 cm) sex difference offset incorporated into the average (i.e., boys vs girls use different offsets).
https://www.aafp.org/pubs/afp/issues/2008/0901/p597.html
A peer-reviewed modeling study reports that incorporating nonlinear corrections (including sex and regression to the mean) can reduce prediction bias substantially and improve variance explained versus simpler mid-parental approaches.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11352326/
Pubertal timing differs by sex: HealthyChildren.org states that on average rapid growth occurs around ~age 11.5 years for girls (range can be earlier/later), and that puberty timing varies substantially among individuals.
https://www.healthychildren.org/English/ages-stages/gradeschool/puberty/Pages/Physical-Development-Whats-Normal-Whats-Not.aspx
HealthyChildren.org notes that, on average, once teens finish puberty, most have gained nearly all of their adult height during puberty and typically grow only another ~1–2 inches afterward.
https://www.healthychildren.org/English/ages-stages/gradeschool/puberty/Pages/Physical-Development-Whats-Normal-Whats-Not.aspx
A clinical reference (Merck Manual Professional Edition) gives typical male pubertal growth-spurt timing: growth spurt occurs between about ages 12 and 16 (for those assigned male at birth not on puberty blockers), with peak typically ages 13–14; >10 cm can be expected in the year of peak velocity.
https://www.msdmanuals.com/en-jp/professional/pediatrics/growth-and-development/physical-growth-and-sexual-maturation-of-adolescents
Johns Hopkins Medicine describes that girls grow an average of about 2–3 inches after menarche, and boys’ growth spurt tends to occur about two years later than girls’ (average pattern).
https://www.hopkinsmedicine.org/health/wellness-and-prevention/what-is-a-growth-spurt-during-puberty
Sleep duration targets (evidence-based public health guidance) from AASM consensus: adolescents (AASM-linked guidance used by AAP) should get about 8–10 hours per night on a regular basis (age 13–18).
https://publications.aap.org/aapnews/news/6630/AAP-endorses-new-recommendations-on-sleep-times
CDC provides a sleep resource page that includes recommended sleep duration ranges (e.g., 8–10 hours per 24 hours for school-age adolescents as reflected in public health guidance).
https://www.cdc.gov/physical-activity-education/staying-healthy/sleep.html
Protein/energy adequacy and micronutrients matter most in children who are not meeting requirements; systematic reviews/meta-analyses report that interventions correcting nutritional deficits can improve linear growth in certain contexts (especially earlier childhood, but also informs general deficiency prevention).
https://www.openurl.ebsco.com/contentitem/doi%3A10.3945/an.116.013938?id=ebsco%3Adoi%3A10.3945%2Fan.116.013938&sid=ebsco%3Acrawler
A systematic review/meta-analysis found zinc supplementation alone showed small positive effects on growth measures in some settings (e.g., under-5 age range in older evidence; results vary by baseline nutrition status).
https://www.ovid.com/journals/tajcn/fulltext/10.3945/ajcn.2008.26862~effects-of-micronutrients-on-growth-of-children-under-5-y-of
AASM pediatric sleep recommendations are based on a formal evidence review, and are intended to avoid health risks of insufficient sleep; while this is not “a guaranteed height increase,” it supports the biological environment for normal development.
https://aasm.org/recharge-with-sleep-pediatric-sleep-recommendations-promoting-optimal-health/
Stretching does not permanently increase bone length/true height; clinical guidance emphasizes stretching helps flexibility/posture rather than changing growth plate outcomes (common myth-debunking point in health systems content).
https://www.goodrx.com/well-being/movement-exercise/does-stretching-make-you-taller
Children’s Hospital resources explain that growth-plate injuries are a known risk in youth sports; this is one mechanism by which sports activities could impair growth indirectly (via injury/recovery).
https://www.childrenscolorado.org/just-ask-childrens/articles/growth-plate-injuries/
HealthyChildren.org highlights “apophysis” and growth-plate-related susceptibility during growth, reinforcing the need for safe training and injury prevention practices.
https://www.healthychildren.org/English/health-issues/injuries-emergencies/sports-injuries/pages/Bone-Injuries-In-Sports.aspx?form=HealthyChildren
For youth athletes, growth spurts are associated with increased injury risk due to rapid musculoskeletal changes; monitoring and supportive training practices are recommended by youth-athlete growth monitoring guidance.
https://youthsports.rutgers.edu/wp-content/uploads/Recommendations-for-Monitoring-and-Supporting-Growth-and-Development-in-Youth-Athletes-By-Eugene-Ketselman.pdf
Precocious puberty is typically defined as onset of puberty signs before age 8 in girls and before age 9 in boys (clinical guideline definition).
https://www.ncbi.nlm.nih.gov/books/NBK279024/
Delayed puberty definitions commonly used in practice include absence of pubertal signs until about age 13 in girls or age 14 in boys (BMJ Best Practice summary of delayed puberty definition).
https://bestpractice.bmj.com/topics/en-gb/1126
Endocrine Society patient guidance on growth-short-stature evaluation notes that clinicians may screen for issues such as anemia, kidney abnormalities, celiac disease sensitivity to gluten, hypothyroidism, and growth/puberty hormone abnormalities.
https://www.endocrine.org/patient-engagement/endocrine-library/growth-and-short-stature
Endocrine Society patient guidance notes that bone age is assessed with an X-ray of the left hand and wrist to determine maturity of growth plates and remaining growth potential.
https://www.endocrine.org/patient-engagement/endocrine-library/growth-and-short-stature
AAFP (short/tall stature evaluation) lists typical initial evaluation components: accurate growth assessment, calculation of growth velocity and midparental height, and bone-age radiography.
https://www.aafp.org/pubs/afp/issues/2015/0701/p43.html
HealthyChildren.org provides examples of chronic conditions that can affect growth (including celiac disease, inflammatory bowel disease, kidney disease, anemia, and others).
https://www.healthychildren.org/English/health-issues/conditions/Glands-Growth-Disorders/Pages/When-a-Child-is-Unusually-Short.aspx
A referral threshold example from a pediatric co-management guideline: projected referral for growth concerns can include height velocity <4 cm/year (annualized) or being >4 inches below mid-parental target height (MPTH) depending on the pathway used.
https://www.legacyhealth.org/-/media/Files/PDF/Services/Children/Diabetes-and-Endocrine/Growth-Short-Stature-and-Failure-to-the-Thrive-CoManagement-Guideline.pdf
AAFP summarizes midparental height as a projected adult height; however, individual outcomes vary and are not guaranteed to match either parent due to genetic variation and population regression effects.
https://www.aafp.org/pubs/afp/issues/2008/0901/p597.html
AAP’s mid-parental method implies a prediction distribution: 95% of children are within about 4 inches above or below the mid-parental calculation, meaning a noticeable share will exceed one parent’s exact height depending on where that parent falls relative to the family midpoint.
https://eqipp.aap.org/courses/growth2/mn/clinical-guide/popups/mid-parental-height
A regression-to-the-mean study framing (reanalysis) discusses how height inheritance data can be explained with regression effects and equal parental contribution in height inheritance models.
https://pubmed.ncbi.nlm.nih.gov/10885190/
A modeling paper on target-height prediction from mid-parental height reports substantial improvements in prediction when correcting for regression to the mean and sex, illustrating that simple “match dad” intuition is limited.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11352326/
A practical reference point for clinicians: HealthyChildren.org states bone-age X-ray is considered the most accurate method among common approaches for predicting adult height (compared with simpler parent-height methods).
https://www.healthychildren.org/English/health-issues/conditions/Glands-Growth-Disorders/Pages/Predicting-a-Childs-Adult-Height.aspx?form=HealthyChildren
AAP EQIPP mid-parental height tool provides an explicit target range: mid-parental height ±10.2 cm and notes that 95% fall within ~4 inches above/below the calculation.
https://eqipp.aap.org/courses/growth2/mn/clinical-guide/popups/mid-parental-height
Children’s Mercy growth failure pathway guidance describes that projected height is determined by extrapolating the child’s current growth curve/channel to the 18–20 year mark on the growth chart and supports endocrinology referral for concerning linear growth velocity patterns.
https://www.childrensmercy.org/health-care-providers/pediatrician-guides/endocrinology/growth-failure/
AAFP notes that initial evaluation should include calculation of growth velocity and midparental height and bone-age radiography to evaluate skeletal maturity.
https://www.aafp.org/pubs/afp/issues/2015/0701/p43.html
Tanner staging (puberty stage) is commonly used clinically to determine pubertal status and interpret growth velocity; the AAP puberty resource emphasizes that pubertal timing and physical development vary by genes and that pediatricians use these patterns to interpret growth.
https://www.healthychildren.org/English/ages-stages/gradeschool/puberty/Pages/Physical-Development-Whats-Normal-Whats-Not.aspx
A pediatric endocrinology guideline-like PDF example lists a referral threshold using growth velocity: strongly recommend referral if growth velocity <4 cm/year for >1 year (and/or other percentile/channel criteria depending on the pathway).
https://assets.contentstack.io/v3/assets/blt7b132cfc09cf5e18/bltbfa07e2e0709f436/2018_Pediatric_Endocrinology_Guidelines.pdf
Next Article
Signs That You Will Not Grow Taller: How to Tell and What to Do
Learn signs you may have stopped growing, how to verify with tracking, and what to do to maximize remaining height poten