If you're searching about Maomao and height growth, you're almost certainly thinking about the protagonist of The Apothecary Diaries. At 17 years old in the story, Maomao is at a stage where most girls are near or past their peak growth window, meaning she likely has very little height left to gain, if any. That said, the real question this raises is a genuinely useful one: how do you actually know whether someone at that age and developmental stage is still growing, and what can influence the outcome? That's where the science gets interesting.
Does Maomao Grow Taller? Growth Plates, Puberty, and What to Do

Marcus Reeves
29 May 2026

Which Maomao are we talking about?
Maomao is the sharp-minded, medicine-obsessed protagonist of The Apothecary Diaries, a manga and light-novel series that got a popular two-season anime adaptation (Season 1 ran October 2023 through March 2024, Season 2 from January through July 2025). She's a young woman trained by her apothecary father, working her way through the politics and mysteries of an imperial inner palace. Character references peg her age at around 17 in the story. There isn't a widely known real person named Maomao in this context, so if you landed here looking for information about a real individual, the biology section below applies to anyone at that age and developmental stage.
How height growth actually works

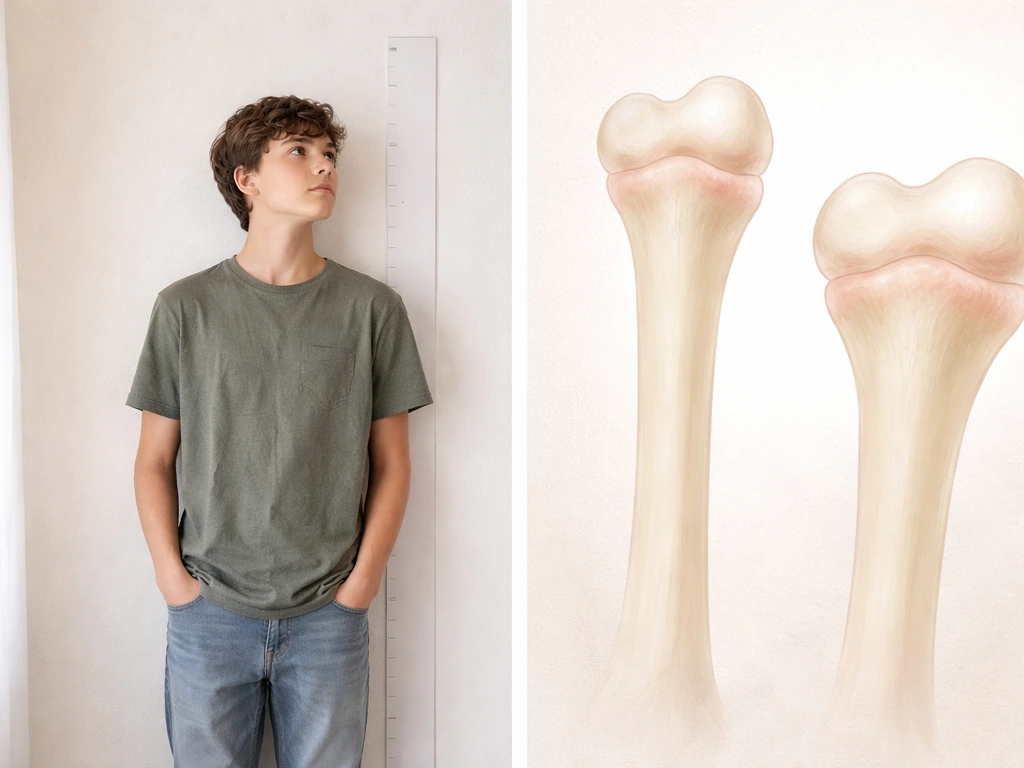
Height increase comes from one place: the epiphyseal plates, commonly called growth plates. These are thin strips of cartilage tissue near the ends of long bones (femur, tibia, humerus, and others) where new bone tissue is generated, pushing the bone longer over time. The key thing to understand is that this process is driven by hormonal signals, primarily growth hormone and IGF-1, and it has a built-in expiration date tied to puberty.
During puberty, the same sex hormones (estrogen and testosterone) that trigger breast development, voice changes, and other maturation events also accelerate bone maturation. That acceleration eventually causes the growth plates to harden and fuse, a process called epiphyseal closure. Wolff's law also explains why appropriate mechanical loading can influence how bones adapt during growth. Once the plates close, the bones can no longer lengthen, and height is essentially locked in. For girls, the peak growth spurt typically happens about 6 to 12 months before the onset of menstruation (menarche), and height gain slows significantly after that point. Most girls finish the majority of their growth within 1 to 2 years of menarche.
Is Maomao still growing at 17?
At 17, most girls are either at the tail end of their growth or have already finished growing. The average age of menarche is around 12 to 13, and since peak growth precedes menarche, most of that height gain happens between 10 and 14. By 17, a girl who went through puberty on a typical timeline has likely been through her main growth spurt for 3 to 5 years already. There may be a small amount of residual growth possible (sometimes up to an inch or so), but the dramatic gains are almost certainly behind her.
That said, late bloomers are real. A person who entered puberty later than average could still be in an active growth window at 17. This is exactly why the question of whether late bloomers grow taller depends on developmental timing, including whether growth plates are still open. This is why clinicians don't just go by age alone. They look at bone age, which is assessed through an X-ray of the left hand and wrist compared against reference atlases of skeletal maturity. A chronological age of 17 paired with a bone age of 14 or 15 indicates meaningful growth potential still remains. Chronological age of 17 with a bone age of 17 to 18 means the plates are nearly or fully closed.
What actually supports healthy height growth
While genetics sets the ceiling (more on that below), several controllable factors meaningfully influence whether someone reaches their genetic potential or falls short of it. These are not magic height boosters; they're the basics that remove obstacles to normal growth.
Nutrition: the foundation

Adequate protein supports the production of growth hormone and IGF-1 and provides the building blocks for new tissue. Calcium is directly incorporated into bone as it lengthens and mineralizes. Vitamin D is critical because without it, calcium cannot be absorbed properly from the gut, and severe deficiency leads to rickets, a condition where bones fail to mineralize correctly and skeletal deformities result. Children and adolescents who are chronically undernourished often end up significantly shorter than their genetic potential would suggest, while correcting deficiencies during the growth window can help restore normal velocity.
Sleep: when growth hormone actually works
Most growth hormone secretion happens during deep sleep, particularly in the first few hours of the night. Chronically short or disrupted sleep during adolescence doesn't just cause fatigue; it cuts into the hormonal environment that drives growth. Age-appropriate sleep targets matter here. Teenagers generally need 8 to 10 hours per night. Consistently getting less than that is a modifiable factor worth addressing, especially during active growth phases. The CDC provides sleep duration recommendations by age, and these targets can be used to support healthy child development Age-appropriate sleep targets matter here.
Physical activity: loading the bones
Weight-bearing exercise and physical activity stimulate bone remodeling and support overall hormonal health during development. There's no specific exercise that "forces" bones to grow longer, but staying physically active supports the hormonal environment that does. Avoid the extreme end here: excessive training with inadequate caloric intake (seen in some elite young athletes) can actually suppress growth by disrupting hormonal balance.
Myths worth clearing up

Once growth plates are fused, no stretching routine, supplement stack, or posture exercise will make you measurably taller in terms of actual bone length. Claims to the contrary are not supported by evidence. What good posture and core strength can do is help you stand at your full existing height rather than losing an inch or two to habitual slouching, which is real and worthwhile, but not the same as growing.
Growth hormone therapy is a legitimate medical treatment for specific diagnosed conditions like growth hormone deficiency or idiopathic short stature in children, and research does show it can increase near-final adult height in carefully selected pediatric patients. But it's not an over-the-counter height hack. It requires pediatric endocrine evaluation, diagnosis, and monitoring. Treating it like a supplement to buy online is both ineffective and potentially dangerous.
- Hanging from a bar does not decompress the spine enough to produce lasting height gains
- Sleeping more after growth plates close does not restart longitudinal bone growth
- Calcium supplements cannot increase height in someone who is already adequately nourished
- Height-increase pills and sprays sold online have no credible clinical evidence behind them
- Yoga and stretching improve flexibility and posture but do not lengthen bones
Estimating realistic height potential and what to do next
The most practical method for estimating a person's genetic height target is the mid-parental height calculation: add both parents' heights together, subtract 5 inches for girls (or add 5 inches for boys), and divide by 2. This gives a midpoint target, with a realistic range of roughly plus or minus 4 inches around it. The American Academy of Pediatrics course module describes a common “target height” approach using mid-parental height with a range of about plus or minus 4 inches (about 10.2 cm) mid-parental height calculation. This is a rough population-level estimate, not a guarantee, but it gives a useful ballpark grounded in family genetics.
To assess whether someone is still actively growing, tracking height measurements over time is more informative than a single reading. Use a stadiometer (the wall-mounted device in a doctor's office) rather than a tape measure or self-measurement, since those methods introduce meaningful error. A normal childhood growth rate is at least about 2 inches (roughly 5 cm) per year. Falling below 4 cm per year in a child who should still be growing is a clinical flag worth discussing with a pediatrician. If there's a concern about stunted or absent growth, a bone age X-ray is the gold-standard tool for determining how much growth potential actually remains. If you suspect you are still in an active growth window, the next step is to confirm it with measurements and, when needed, a bone age X-ray can still grow taller.
For Maomao specifically as a fictional character, the in-universe answer is that at 17 she is almost certainly at or near the end of her growth window, with only modest additional height gain possible if she's a late developer. For anyone in the real world asking this question about themselves or someone they know at a similar age: check where you are in puberty development, get an accurate height measurement, track it over 6 to 12 months, and focus on the fundamentals of sleep, nutrition, and activity. So if you're asking, "does asta grow taller," the key is to check where puberty and growth plates stand, because height potential is limited by developmental timing. If growth seems abnormally slow for the developmental stage, that's a conversation worth having with a pediatric endocrinologist rather than something to try to fix with supplements. The biology here is well understood, and good medical assessment is far more useful than guesswork.
| Factor | Matters for growth? | Works after plates close? |
|---|---|---|
| Adequate protein intake | Yes, supports GH and IGF-1 | No height effect |
| Calcium and vitamin D | Yes, critical for bone mineralization | Supports bone density, not height |
| Sleep (8-10 hrs for teens) | Yes, peak GH secretion during sleep | No height effect |
| Weight-bearing exercise | Yes, supports bone remodeling | No height effect |
| Stretching / hanging | No evidence for height gain | No height effect |
| Growth hormone therapy | Yes, for diagnosed GHD/ISS under medical care | Not indicated for adults without deficiency |
The broader question of whether someone can still grow taller connects to a lot of related biology worth understanding. Whether you're looking at late developers who may still be in an active window, or thinking about the mechanical principles of how bones respond to load over time, the same core principle applies: growth potential is time-limited and biologically anchored to developmental stage, not just age on paper. Getting that assessment right is the starting point for any realistic plan.
FAQ
How can I tell if my growth plates are still open if I am already 16 or 17?
Age alone is not reliable. The practical approach is to combine puberty timing with tracking growth over time, then confirm with a bone age X-ray if there is concern. For many people, a big clue is whether menstruation started recently (peak growth typically happens before it), and whether measured height is still increasing at a normal rate (roughly at least 5 cm per year in childhood and early adolescence).
If I do not grow for a few months, does that mean I will never get taller?
Not necessarily. Height can pause briefly due to illness, changes in sleep, appetite, or training load, and measurement variation is common at home. Clinicians usually look at a 6 to 12 month trend using consistent measurement methods. A single slow interval is less informative than the overall trajectory.
Are home stadiometer measurements good enough, or should I wait for a doctor’s measurement?
Home measurements can be useful if done carefully, but they introduce more error than a clinical stadiometer, especially if you use a tape or uneven surfaces. To get meaningful trend data at home, measure at the same time of day, keep posture consistent, and record the same method each time. If the result is borderline or concerning, confirm in clinic.
What is the fastest way to spot a growth problem that deserves a pediatric endocrinology visit?
A common red flag is growth that is clearly slower than expected for the developmental stage, such as a long period below about 4 cm per year in a child who should still be growing, or crossing growth percentiles downward on a growth chart. Another reason to seek evaluation is puberty timing that seems far outside typical ranges (very early or very late), especially if height acceleration or expected growth spurt never happened.
Can posture exercises or stretching make me taller in the real sense?
They can improve how tall you look by reducing slouch, which may add a small amount of visible height, but they do not lengthen fused bone. If growth plates are closed, true height gain is not expected from posture routines, and you should treat “taller overnight” claims as unreliable.
Do weight and diet changes during teen years affect height even if I am close to finishing puberty?
Yes. Even near the end of growth, chronically low calorie intake and poor protein can reduce growth velocity or contribute to delayed puberty. The key is not extreme dieting, and not relying on supplement stacks. If intake has been insufficient or weight has dropped quickly, correcting nutrition can help you avoid missing remaining potential.
What sleep schedule actually matters for height during adolescence?
Consistency matters more than occasional late nights. Growth hormone secretion rises during deep sleep, especially early in the night, so a bedtime that allows adequate total sleep is important. Many teens do best with about 8 to 10 hours nightly, and ongoing short sleep is a modifiable factor worth addressing.
If my parents are short, is it still possible to reach my genetic target, or is it hopeless?
It is not hopeless, but the genetics “ceiling” is real. Your mid-parental estimate provides a rough target range, yet modifiable factors like adequate nutrition, vitamin D status, and healthy sleep can determine how much of that range you realize. The most actionable step is to check whether you are still in an active growth window rather than assuming genetics is the whole story.
Is growth hormone therapy an option for someone who is already a late teen?
Growth hormone therapy is typically considered for children and adolescents with specific diagnosed conditions, and it requires pediatric endocrine evaluation and monitoring. If growth plates are nearly closed or bone age suggests limited remaining growth, the benefit is often small, which is why bone age and diagnosis matter before pursuing treatment.
How does late puberty change the likelihood of gaining a little height after 17?
Later puberty can mean growth plates remain open longer, so some additional growth may occur after 17 compared with someone who had early puberty. However, the amount varies, and measuring growth over 6 to 12 months plus checking bone age gives the most useful estimate of whether the remaining window is meaningful.
Next Article
Does Asta Grow Taller? Realistic Growth Chances by Age
Find out if Asta can still grow taller by age, puberty stage, growth plates, and practical steps to support height.