Yes, late bloomers often do end up taller than early bloomers, but the reason is more nuanced than most people realize. It is not simply that starting puberty later gives you more growing time. The biology behind it involves growth plate timing, hormonal exposure, and genetic ceiling, and understanding those pieces will tell you a lot more about your own situation than any rule of thumb will.
Do Late Bloomers Grow Taller Than Early Bloomers?

Marcus Reeves
19 Apr 2026

What 'late bloomer' actually means for height

In the context of height and growth, a late bloomer is someone whose puberty, and with it their major growth spurt, starts later than average. Clinically, doctors start paying attention when a girl shows no breast development by age 13 or a boy shows no testicular enlargement by age 14.
Those are the standard cutoffs used to flag possible delayed puberty for evaluation. But 'late bloomer' in everyday use is broader than that. Plenty of kids who start puberty at 12 or 13 (instead of the more common 10 or 11) think of themselves as late bloomers even though they are technically within the normal range. The key point is the same either way: their peak height velocity, the period of fastest growth, comes later than their peers.
It is worth separating two things that sometimes get confused. 'Late bloomer' usually refers to the timing of puberty, not to constitutional short stature or a growth disorder. A child can be completely normal and healthy and simply have a family pattern of later puberty. That pattern even has a clinical name: constitutional delay of growth and puberty (CDGP). It is the most common reason a teenager is shorter than classmates at 14 or 15, and it usually resolves on its own with a late growth spurt.
Do late bloomers end up taller, and why does timing matter?
On average, yes, people who go through puberty later tend to reach adult heights that are similar to or slightly taller than early bloomers from comparable genetic backgrounds. The comparison can be misleading in adolescence because a 14-year-old early bloomer often looks significantly taller than a same-age late bloomer. By 18 to 20, that gap usually closes, and sometimes reverses.
Why? Because the growth spurt tied to puberty is time-limited. Once sex hormones (estrogen and testosterone) rise substantially, they trigger the gradual closure of growth plates. An early bloomer gets the spurt sooner but also closes out sooner. A late bloomer's growth plates remain open and active longer, meaning more total growth time even if the spurt itself arrives late. The genetic height potential that was always in the blueprint gets more runway to be expressed.
That said, timing alone does not determine final height. Genetics sets the ceiling, and nutrition, health, and sleep determine how close to that ceiling a person actually gets. Two people with the same late-bloomer pattern can end up at meaningfully different heights depending on those factors. Timing matters, but it is one variable among several.
The biology behind it: growth plates, hormones, and growth spurts
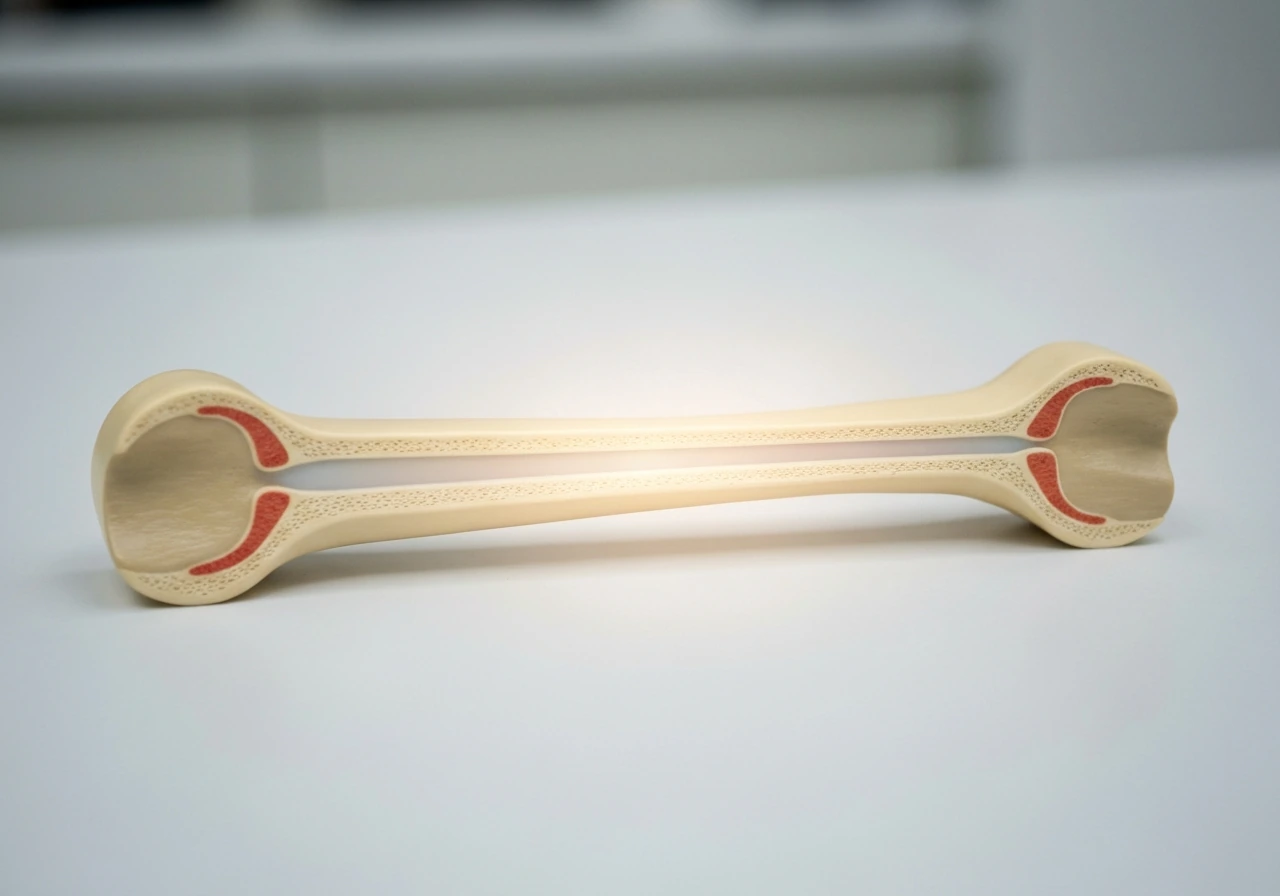
Long bones grow at regions called epiphyseal plates, or growth plates, located near the ends of bones like the femur and tibia. These plates are made of cartilage that is continuously replaced by new bone tissue, pushing the bone longer. As long as those plates remain open (unfused), height growth is possible.
Puberty triggers a surge in growth hormone, IGF-1, and sex steroids, which first accelerates growth (the growth spurt) and then, over time, causes the plates to fuse. Early puberty means earlier fusion. Later puberty means the plates stay open longer, which extends the window in which real height can be added. A late bloomer at age 15 may still have wide-open growth plates while a same-age early bloomer's plates are already partially or fully fused. Bone age assessments (X-rays of the wrist or hand) can confirm this, and they are a standard part of evaluating suspected delayed puberty alongside hormone tests for LH, FSH, testosterone or estradiol, and thyroid function.
The growth spurt itself in late bloomers tends to be just as robust as in early bloomers, sometimes more so, because the body has had more time accumulating pre-pubertal growth and the hormonal surge is sharp when it finally arrives. Peak height velocity during puberty in males typically hits around 4 inches (10 cm) per year, and in females around 3 inches (7.5 cm) per year, regardless of whether puberty started at 11 or 15.
Male late bloomers vs. early bloomers: the sex-specific picture
This question comes up most often for boys, and for good reason. Male puberty has a wider normal timing range than female puberty, and the social visibility of height differences in teenage boys is intense. A boy who is still prepubertal at 15 can be 5 to 6 inches shorter than classmates who started puberty at 12, even if both will ultimately land near the same adult height.
For males, late puberty onset (defined clinically as no testicular enlargement by age 14) often means the growth spurt hits between ages 15 and 18 instead of the more typical 12 to 15. Boys have a longer pre-pubertal growth period in general, which is partly why the average male adult height exceeds the average female adult height. A male late bloomer can still be growing meaningfully at 18 or even 19, while an early bloomer may have finished by 16. That extra growth window is real and significant.
Constitutional delay of growth and puberty (CDGP) is also more commonly diagnosed in boys than girls, partly because the social stakes of late development are more noticeable in male adolescence. Family history matters here: if a boy's father or uncles were late developers who eventually caught up, the odds that this is CDGP (rather than a pathological delay) are high. A bone age X-ray showing delayed skeletal maturation alongside normal growth velocity is generally reassuring.
Can early bloomers grow tall too? What height really depends on
Absolutely. Early puberty does not automatically mean short adult stature. Plenty of people who hit puberty at 10 or 11 grow to above-average heights, because genetics, nutrition, and overall health are doing most of the work. A child with tall parents and excellent nutrition who starts puberty early may well surpass a late bloomer from a shorter family. The genetic ceiling is the primary driver of final height, and timing is one factor that influences how close a person gets to it.
Early bloomers do tend to have a shorter growth window after puberty, but if their genetic potential is high and they have the nutrition and health to support it, they can absolutely reach tall heights. The risk for early bloomers is that precocious puberty (puberty starting well before the typical range, especially before age 8 in girls or 9 in boys) can actually limit adult height by closing growth plates prematurely. That is a different clinical situation from simply being an early-normal developer, and it sometimes warrants treatment to preserve growth potential.
The bottom line: height is not a race won by late bloomers or early bloomers. It is determined by genetic potential, how well the body is supported during the entire growth period, and whether any medical factors are interfering with normal development. Timing is one piece of the puzzle, and an important one, but it is not the whole story.
Related questions about whether general growth is still possible in various circumstances are worth exploring as part of the broader picture. For a related example of how growth timing can affect height, see does maomao grow taller. Related questions about whether general growth is still possible in various circumstances are worth exploring as part of the broader picture does asta grow taller.
How to maximize your remaining height potential right now
If you are still growing, or think you might be, the basics matter enormously. There is no supplement or trick that overrides biology, but there are well-documented ways to ensure you are not leaving height on the table due to avoidable deficiencies or poor habits.
Sleep
Growth hormone is released primarily during deep sleep, with the largest pulse happening in the first few hours after falling asleep. Teenagers need 8 to 10 hours of sleep per night, and consistently getting less than 7 is a real risk factor for blunted growth hormone output. This is not a minor point. Sleep is arguably the single most underrated factor in adolescent growth, and it is entirely within your control.
Nutrition: calories, protein, and key micronutrients

Adequate calories matter first. Chronic undereating, even without a diagnosed eating disorder, suppresses growth hormone and IGF-1 and can stall height growth. During the growth spurt, caloric needs spike significantly. Beyond total calories, protein is critical: it provides the amino acids used to build bone and muscle during growth, and protein deficiency in childhood and adolescence is one of the clearest documented causes of reduced height potential worldwide.
Calcium and vitamin D work together to support bone mineralization. The recommended intake for adolescents is around 1,300 mg of calcium per day and at least 600 IU of vitamin D, though many teens are deficient in vitamin D especially in northern latitudes or with limited sun exposure. Zinc is another micronutrient tied to growth, and deficiency has been linked to delayed puberty and growth stunting. A reasonable varied diet rich in dairy or fortified alternatives, lean protein, leafy greens, and whole grains covers most of these bases without supplementation for most healthy teens.
Exercise
Regular physical activity stimulates blank" rel="noopener noreferrer">growth hormone release and supports bone density. Weight-bearing exercise (running, jumping, team sports, resistance training with appropriate form and load) is beneficial during growth years. Wolff's law also explains why the right mechanical loading can help stimulate bone strength during the growth years. There is no credible evidence that resistance training stunts growth in adolescents when done correctly. The old myth about lifting weights being dangerous for growing kids has not held up to scientific scrutiny. What matters is avoiding extremely heavy maximal loads on an immature skeleton and ensuring proper technique.
Posture
Posture will not make you grow taller in the biological sense, but significant postural problems like pronounced forward head posture or thoracic kyphosis can make you appear shorter than your actual skeletal height. Correcting these through core strengthening, back exercises, and body awareness can recover 0.5 to 2 inches of visible height in some people. It is not growth, but it is real height that was being hidden.
Medical timing and intervention
If there is a reason to suspect a medical issue is delaying or disrupting puberty, timing matters. Conditions like hypothyroidism, celiac disease, inflammatory bowel disease, and growth hormone deficiency can all suppress height growth, and the earlier they are identified and treated, the more growth potential is preserved. Waiting too long to evaluate a genuine problem means fewer open growth plates to work with.
When to track growth and when to see a doctor

If you are monitoring a child or teenager, growth velocity matters more than a single height measurement. A child who is consistently growing 2 to 2.5 inches (5 to 6 cm) per year before puberty is likely on track, even if they are shorter than peers. A child who has slowed significantly below normal growth velocity for their age and pubertal stage warrants attention, regardless of where they fall on the height chart.
Standard pediatric growth charts (CDC or WHO versions) plot height for age and sex as percentiles. Crossing percentile lines downward over time, or sitting below the 3rd percentile, is more clinically meaningful than being short relative to friends. Your pediatrician should be plotting these at every well-child visit. If they are not, ask.
Seeing a pediatric endocrinologist makes sense in these scenarios:
- A girl shows no breast development by age 13 or a boy shows no signs of testicular enlargement by age 14
- Growth velocity has slowed significantly or stopped unexpectedly
- A child has dropped two or more major percentile lines on the growth chart
- There are other symptoms suggesting hormonal or systemic illness (fatigue, weight changes, delayed milestones)
- A teenager is significantly distressed by delayed puberty and height, even if a pathological cause is not yet established
A pediatric endocrinologist will typically order a bone age X-ray (a left hand and wrist X-ray that estimates skeletal maturity), blood tests including LH, FSH, testosterone or estradiol, thyroid function, and sometimes IGF-1 and growth hormone stimulation tests when deficiency is suspected. This workup distinguishes constitutional delay (a normal variant that just needs time) from conditions that require treatment. That distinction is important: constitutional delay usually needs only watchful waiting and sometimes short-term intervention, while true hormonal deficiencies or systemic diseases need specific treatment.
If the evaluation confirms constitutional delay, the realistic expectation is that the growth spurt will arrive and the person will reach close to their genetic height potential. Mid-parental height calculation (averaging parents' heights with a correction for sex) gives a reasonable target range, typically plus or minus 4 inches (10 cm) around that midpoint. Most late bloomers with CDGP land within that range once they finish growing.
| Factor | Early Bloomers | Late Bloomers |
|---|---|---|
| Puberty onset | Earlier (girls ~9-11, boys ~10-12) | Later (girls ~12-14, boys ~13-16) |
| Growth spurt timing | Earlier peak height velocity | Later peak height velocity |
| Growth plate closure | Earlier fusion | Later fusion, longer growth window |
| Height during mid-adolescence | Often taller than peers | Often shorter than peers temporarily |
| Final adult height | Reaches genetic potential early | Often catches up, sometimes exceeds early bloomers |
| Main risk to height potential | Precocious puberty closing plates too soon | Underlying illness masquerading as late puberty |
The practical takeaway: if you or a teenager you care about is a late bloomer, the odds are genuinely on your side for reaching full genetic height, sometimes after peers have already stopped growing. Support that process with solid sleep, adequate nutrition, regular exercise, and appropriate medical follow-up. Do not assume short stature at 15 or 16 is the end of the story, because for many late bloomers, it very much is not.
FAQ
Does starting puberty late mean I will definitely be taller than early bloomers as an adult?
Not definitely. Late puberty can extend the time for growth, but final height still depends on genetics (your height ceiling), overall nutrition, chronic illness, and sleep quality. Two people with the same delayed timing can end up noticeably different if one has better health or fewer growth-disrupting issues.
If I am a late bloomer at 15, can I still grow after 18?
Often yes, especially for boys, because male growth typically lags longer and growth plates can remain open into the later teen years. A practical check is bone age, since it estimates skeletal maturity and helps predict whether meaningful growth is still likely.
Can someone be a “late bloomer” and still have a growth disorder?
Yes. Delayed puberty timing can be constitutional (CDGP), but it can also be due to problems like hypothyroidism, celiac disease, inflammatory bowel disease, or growth hormone deficiency. The key distinction is not just how late puberty starts, but whether growth velocity and labs look normal for the child’s stage.
What growth rate should make me pay attention even if puberty seems delayed?
Use growth velocity and trend, not one measurement. As a rough guide from pediatric practice, steady pre-pubertal growth is often around 2 to 2.5 inches (5 to 6 cm) per year, and a significant slowing below that for age and pubertal stage is a reason to get evaluated.
How can early bloomers end up tall if their growth window closes sooner?
If their genetic height potential is high and they maintain strong sleep, adequate calories, and enough protein, they may reach above-average adult height despite an earlier spurt. Early timing only shortens the window, it does not automatically reduce the final ceiling set by genetics.
Does puberty being “early” always cause short adult height?
No. Early onset within normal limits does not guarantee short stature. The concern is more specific for true precocious puberty (especially starting well before typical ages), because it can close growth plates early. That scenario may warrant treatment to preserve remaining growth potential.
If growth plates are still open, will that guarantee more height gain?
Open growth plates are necessary but not sufficient. You also need adequate hormonal signaling and sufficient building blocks, meaning calories, protein, and key micronutrients, plus no chronic condition suppressing growth. Bone age can show plate status, but growth velocity and overall health show whether the body can use that remaining time.
Should I focus on posture if I think I am not growing taller?
Posture changes can affect how tall you look, especially if kyphosis or forward head posture is present, but it will not increase true bone length. If you suspect a posture issue, core and back strengthening can improve visible height, but ongoing growth delay still needs growth-velocity evaluation.
Does resistance training affect whether I grow taller?
When done with proper technique and appropriate loads, resistance training is not credibly shown to stunt growth. The bigger practical risk is using extremely heavy maximal loads on an immature skeleton, so supervised, progressive training is the safer approach.
What is the most common avoidable reason teens do not reach their potential height?
Consistently insufficient sleep and inadequate calories or protein. Growth hormone pulses are highest in deep sleep, and chronic under-eating can blunt growth-related hormones like IGF-1, which reduces growth even if timing of puberty is otherwise favorable.
When is it worth asking for medical evaluation rather than waiting?
If puberty appears delayed based on standard clinical cutoffs, or if growth velocity drops significantly for age and stage, evaluation is usually worthwhile. Waiting too long can reduce remaining open growth plate time if a real medical cause is present, so earlier assessment often helps.
Next Article
What Amino Acids Make You Grow Taller
Know which amino acids support growth via protein and IGF-1, why they can’t extend height after closure, and practical t
