Eating more food will not automatically make you taller, but eating too little of the right nutrients absolutely can hold back your growth if your body still has the capacity to grow. The key variable is whether your growth plates are still open. If you're a child or teenager in active development, nutrition plays a meaningful role in reaching your genetic height potential. If you're an adult with fused growth plates, no amount of food will add inches to your frame. The relationship between eating and height is really about quality, timing, and specific nutrients, not just calories.
Will I Grow Taller If I Eat More? Nutrition, Sleep, Myths

Marcus Reeves
15 Jun 2026

How height growth actually works
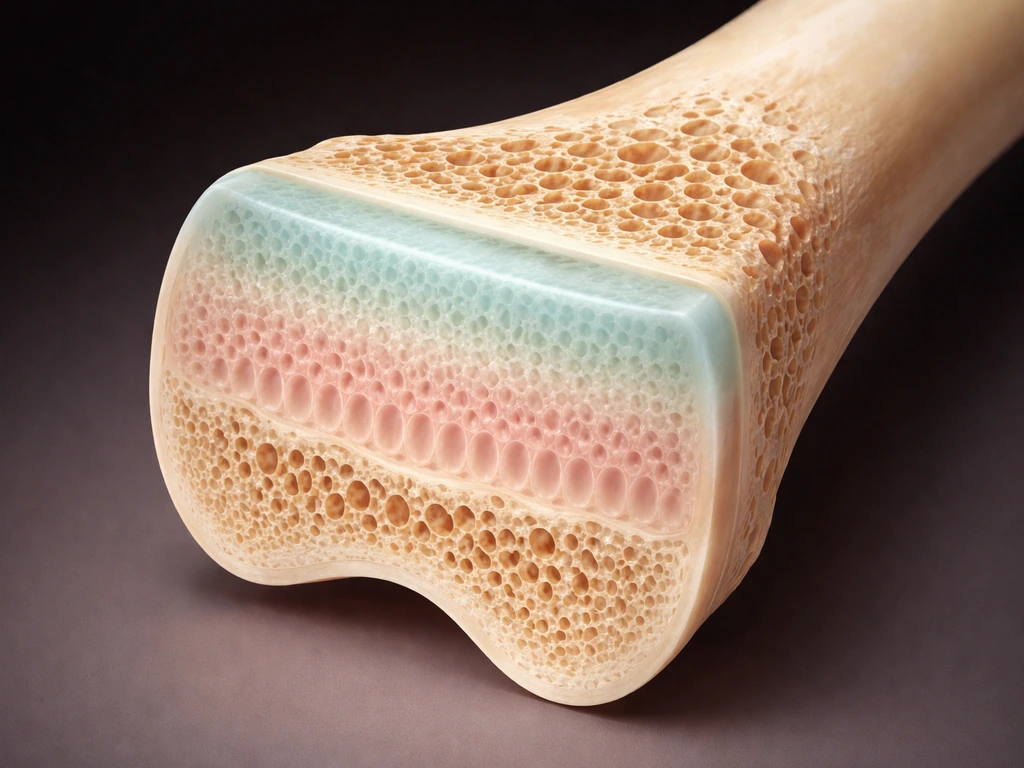
Your bones grow longer at structures called epiphyseal growth plates, sometimes called the physis. These are zones of cartilage near the ends of your long bones, like the femur and tibia, that stay active throughout childhood and adolescence. Specialized cells in these plates, called chondrocytes, multiply and produce extracellular matrix that eventually mineralizes into new bone, pushing bone ends further apart and making you taller.
The main hormonal driver of this whole process is the growth hormone and IGF-1 axis. Your pituitary gland releases growth hormone (GH), which then stimulates the liver and local tissues to produce insulin-like growth factor 1 (IGF-1). IGF-1 acts directly on the chondrocytes in the growth plate, triggering them to grow and multiply. During puberty, sex steroids cause GH secretion to increase roughly 1.5 to 3 times compared to pre-puberty levels, and serum IGF-1 concentrations jump more than 3-fold. This is the engine behind the adolescent growth spurt.
Eventually, those same sex hormones that drive the growth spurt also signal the growth plates to ossify and fuse. Once the growth plates close, linear growth stops permanently. MRI research shows that most growth plates are fully fused by ages 17 to 19, with females typically completing fusion about two years earlier than males on average, though there is meaningful individual variation from bone to bone and person to person.
What nutrition can and can't do for height
Nutrition's influence on height is real but conditional. The clearest evidence comes from situations of significant undernutrition: children who are chronically underfed or deficient in key micronutrients often experience stunted growth, and correcting those deficiencies can partially restore normal growth velocity. The WHO recognizes malnutrition as a major cause of stunting globally. But the flip side of that is important: once you're meeting your nutritional needs adequately, adding more food beyond that threshold doesn't push you past your genetically encoded ceiling.
Think of it this way. Genetics set the upper limit for your height. Nutrition, along with sleep and overall health, determines how close you actually get to that limit. If everything is adequate, you'll likely reach your genetic potential. If something is deficient, you may fall short of it. But surplus eating beyond adequacy doesn't stretch that ceiling higher. Effect of preventive zinc supplementation on linear growth in children under 5 years of age notes that preventive zinc supplementation (systematic review/meta-analysis input for the Lives Saved Tool) reported that zinc supplementation is associated with a net benefit on linear growth and that a preventive dose of 10 mg/day had the most significant effect on linear length in children <5 years (mean difference reported ~0.46 cm).
The evidence here is nuanced. Systematic reviews of nutritional interventions in children beyond age two have found that not all nutrients affect linear growth equally. Calcium-containing interventions, for instance, haven't shown clear evidence of improving linear growth as a public health strategy in that evidence synthesis, even though calcium is critical for bone density. Similarly, iron supplementation has not consistently shown benefits for linear growth, particularly in developed-country settings. The nutrients with the strongest evidence for linear growth effects in deficient populations are zinc, protein, and multiple micronutrient combinations.
Why just "eating more" doesn't make you taller

There's a common assumption, especially among teens trying to bulk up or gain muscle, that more food equals more growth in every direction. That's not how it works. Height growth depends on your growth plates being active, your hormonal environment being functional, and specific building blocks being available. Simply eating extra calories, especially in the form of processed food or excess macronutrients without micronutrient density, doesn't give the growth plate the signals or substrates it needs.
What growth requires is not caloric excess but caloric sufficiency paired with micronutrient adequacy. If you're a teenager eating 3,000 calories a day of mostly ultra-processed food, you may still be zinc-deficient or vitamin D-deficient, both of which can blunt growth. Conversely, a teenager eating 2,200 well-structured calories with adequate protein, zinc, and vitamin D is giving their body what it actually needs to build height. Volume alone is a poor proxy for nutritional quality.
There's also the question of energy deficit. Chronic undereating, which is common in athletes, kids with restrictive eating, or families facing food insecurity, can suppress growth hormone release and reduce IGF-1 levels, directly slowing growth plate activity. So while excess calories don't help, genuinely inadequate energy intake does hurt. The goal is to make sure you're not in a meaningful deficit, not to eat beyond your needs.
The nutrients that actually matter for growth
Rather than trying to eat more of everything, focus on getting enough of the specific nutrients with the strongest links to growth and bone development. Here's how the evidence breaks down:
| Nutrient | Role in Growth | Evidence Strength | Practical Sources |
|---|---|---|---|
| Protein | Provides amino acids for IGF-1 production and collagen synthesis in bone/cartilage | Strong for deficient populations | Meat, fish, eggs, legumes, dairy |
| Zinc | Supports cell division and growth hormone signaling; deficiency is linked to stunting | Strong; ~0.46 cm benefit in deficient children under 5 at 10 mg/day | Red meat, shellfish, seeds, legumes, nuts |
| Vitamin D | Supports calcium absorption and bone metabolism; deficiency is common globally | Moderate; clearest benefit when correcting deficiency | Sunlight, fatty fish, fortified dairy, supplements |
| Calcium | Critical for bone mineral content but limited direct evidence for linear growth | Weaker for height specifically; strong for bone density | Dairy, leafy greens, fortified foods |
| Iron | Supports overall health and development; deficiency impairs many physiological processes | Limited for linear growth specifically | Red meat, beans, fortified cereals, spinach |
| Vitamin A | Involved in multiple micronutrient interventions that showed positive height effects | Moderate as part of combined interventions | Liver, eggs, orange/yellow vegetables |
Zinc stands out as particularly well-supported for linear growth in children. Preventive zinc supplementation at around 10 mg per day has shown a measurable mean difference in linear length in children under five who were deficient. Protein is similarly foundational because the GH/IGF-1 axis needs adequate amino acids to function properly. Vitamin D matters most when baseline levels are genuinely low, which is surprisingly common even in well-fed populations due to limited sun exposure. If you're concerned about a child's growth, getting bloodwork to check for these deficiencies is a much better starting point than simply adding more food.
Sleep and daily habits that work alongside food

Growth hormone is not released at a steady rate throughout the day. The largest pulses happen during deep slow-wave sleep, typically in the first few hours after falling asleep. This means sleep quantity and quality directly affect how much GH your body produces each night. For children and teenagers especially, consistently shortchanging sleep is not just a tiredness issue, it's a physiological one that affects the hormonal environment needed for growth.
The American Academy of Sleep Medicine recommends the following sleep durations by age group:
- Ages 3 to 5: 10 to 13 hours per 24 hours, including naps
- Ages 6 to 12: 9 to 12 hours per night
- Ages 13 to 18: 8 to 10 hours per night
One practical obstacle here is screen use before bed. Research following early adolescents over time has found that bedtime screen use is associated with shorter sleep duration and more sleep disturbance up to a year later. Cutting screens 30 to 60 minutes before bed is one of the highest-leverage habits for protecting sleep quality during the years when growth hormone is most active. It sounds simple, but the data support taking it seriously.
Stress management also matters, though it's harder to quantify. Chronic psychological stress elevates cortisol, which can suppress GH secretion and have downstream effects on IGF-1. This is one reason why children in chronically stressful or unstable environments sometimes show growth faltering that doesn't track with their caloric intake alone.
Exercise and how it interacts with growth
Exercise during childhood and adolescence supports bone development, but its direct effect on height is modest and mostly works through bone health rather than pushing you past your genetic ceiling. Systematic reviews show that exercise is generally associated with osteogenic (bone-building) effects during adolescent growth, particularly improving bone mineral density and content. This matters for long-term skeletal health but is distinct from adding centimeters to your height.
One concern that comes up is whether intense exercise, particularly resistance training, can damage growth plates in young people. The evidence from prospective studies where training is properly supervised and age-appropriate has not reported growth plate injury. The risks appear concentrated in unsupervised, excessive loading situations, not structured, appropriate resistance training. So weight training during teen years is not something to avoid out of fear of stunted growth, as long as it's done properly.
The situation that genuinely can impair growth is the opposite: too much training combined with too little food. This is captured by the concept of Relative Energy Deficiency in Sport (RED-S), where low energy availability suppresses hormonal systems including GH and IGF-1 signaling, compromises bone health, and can have lasting effects on growth in still-developing athletes. Young athletes in sports with weight categories or aesthetic emphasis are particularly vulnerable. If a teenager is training hard but eating too little, that combination is more harmful than either factor alone.
What to actually do with exercise for growth support: prioritize activities that involve some loading impact (running, jumping, general athletics) to stimulate bone adaptation, include structured resistance training with appropriate guidance, and make sure caloric and nutrient intake matches the energy demands of the training load.
Timing matters: children and teens vs. adults
This is probably the most important context for anyone reading this. Everything discussed about nutrition and growth applies specifically to people whose growth plates are still open. Once they close, the game changes completely.
For children still in their growth years, clinicians track not just height but growth velocity, meaning how fast they're growing per year. A healthy growth rate is generally considered at least about 2 inches (5 cm) per year in childhood, though this varies by age and stage of puberty. If a child is growing consistently and on track with their growth curve percentile, nutrition adjustments are about optimization, not rescue. If a child is dropping across percentile lines on their growth chart or not growing at expected velocity, that warrants a medical evaluation, not just more food.
For teenagers, the window is narrowing. The pubertal growth spurt typically peaks early in puberty (earlier for girls, later for boys) and then tapers off as sex hormones trigger growth plate fusion. By the time most girls reach 15 to 16 and most boys reach 17 to 18, the majority of linear growth is done. Optimizing nutrition and sleep during the earlier teen years has more leverage than trying to intervene at the tail end of puberty. Growth and Short Stature | Endocrine Society notes that poor height growth rate/growth velocity is described clinically as failing to grow at least ~2 inches per year and/or dropping across height percentiles on the growth chart in patient-facing guidance.
For adults with fully fused growth plates, eating more will not make you taller. Full stop. The cartilaginous plates that would need to be active are gone, replaced by bone. What adults can do is optimize posture (which affects apparent height), maintain bone density through adequate calcium, vitamin D, and weight-bearing exercise to prevent height loss with age, and ensure they're not dealing with a nutrient deficiency that might affect overall health and vitality.
If you're wondering whether you or your child still has growth potential, factors like signs of active puberty, bone age assessment (a wrist X-ray a pediatrician can order), and family history of late growth all help clarify the picture. These signs of active growth potential matter, because they can indicate whether you will grow taller as your growth plates remain open sign you will grow taller. These questions about whether growth potential remains open are worth exploring with a pediatric endocrinologist if there's any real concern.
How to actually assess and improve your nutritional intake for growth
Rather than guessing, here's a practical approach to figure out whether your diet might be limiting your growth potential:
- Get bloodwork done: Ask a doctor to check serum 25(OH)D (vitamin D status), zinc, ferritin (iron stores), and a basic metabolic panel. This tells you whether you have actual deficiencies to correct rather than just guessing.
- Track your protein intake for a few days: Growing children and teens need roughly 0.8 to 1.2 grams of protein per kilogram of body weight daily, sometimes more for active individuals. Many teens undershoot this without realizing it.
- Assess energy adequacy: If you're consistently tired, not recovering from exercise, or feeling cold, you may be in a chronic mild energy deficit. Tools like a registered dietitian or a simple food diary can help identify this.
- Build meals around nutrient density, not just volume: A meal of lean protein, vegetables, whole grains, and a dairy or calcium-rich food covers most of the key growth-related nutrients without requiring huge quantities of food.
- Prioritize sleep hygiene as seriously as diet: Set a consistent bedtime, reduce screen exposure in the hour before sleep, and aim for the AASM age-appropriate sleep duration ranges listed above.
- Talk to a clinician if growth seems slow: If a child isn't reaching expected height milestones, is dropping growth chart percentiles, or shows signs of delayed puberty, get a medical evaluation before assuming it's purely a dietary fix.
Setting realistic expectations
The honest summary is this: if you're a child or teenager with open growth plates, making sure you're eating enough of the right nutrients, sleeping well, staying active, and managing stress gives you the best chance of reaching your genetic height potential. If you quit smoking, you may improve overall health and circulation, but it won't reopen closed growth plates or guarantee extra inches. If you're wondering, "do i have a chance to grow taller," the key is whether your growth plates are still open and your nutrition, sleep, and health are supporting that potential. Doing all of this perfectly still won't make you taller than your genes allow, but it prevents you from falling short of that potential due to something avoidable. For adults, the focus shifts from growing taller to maintaining the height you have by protecting bone health over time.
Height is also just one signal worth paying attention to. Growth velocity, how you feel, energy levels, bone health, and overall development give a much fuller picture than a single number on a measuring tape. If you have real concerns about whether you or your child has growth potential that remains open, or signs that point to a sign of ongoing growth, exploring the specific factors, from genetics to nutrition to hormonal health, with a clinician is the most useful next step you can take.
FAQ
If I eat more and my weight increases, will I automatically get taller too?
Not necessarily. If you are already meeting your calorie and micronutrient needs, extra calories mostly increase body weight, not length. Height gains still require open growth plates and enough specific inputs, especially protein and zinc, and adequate vitamin D if your levels are low.
Can I “make up” lost height by eating better later?
Catch-up is possible mainly when growth is being limited by undernutrition, chronic deficiency, or energy deficit, and when growth plates are still open. It tends to show up as improved growth velocity over months, so the right metric is whether your annual height gain moves back toward your expected growth curve, not the short-term scale change.
As an adult, what changes can happen if I improve my diet and eat more?
If you are an adult, you cannot lengthen bones because growth plates are fused. What you may notice instead is improved posture, reduced spinal compression, and better bone health, which can change how tall you appear (sometimes by a small amount) but not true bone length.
How much should a teen increase calories to support height, without overdoing it?
You do not need to target extreme amounts. Overeating can crowd out nutrient-dense foods, increase total processed food intake, and make micronutrient gaps more likely. The practical goal is meeting your calorie needs without chronic restriction and ensuring zinc, protein, and vitamin D adequacy.
If my child’s diet changes, how soon should we see effects on height?
A short-term growth spurt might not align with how much you ate that week. Growth responds over time to overall energy balance, nutrient sufficiency, sleep timing, and hormonal rhythm. The best indicator is growth velocity on a chart over repeated measurements, ideally every 3 to 6 months for kids and teens if there are concerns.
What if my child eats enough calories, could they still be missing something that affects height?
Not all deficiencies show up with the same diet pattern. For example, a “healthy” diet can still be low in vitamin D due to limited sun exposure, and high-calorie ultra-processed diets can still be low in zinc or protein. If growth concerns exist, bloodwork can distinguish missing nutrients from other causes.
Should I supplement iron to help my child grow taller?
Iron is important for overall health, but iron supplementation does not reliably increase linear growth in everyone. If someone is deficient, treating the deficiency is worthwhile, but for growth specifically, zinc, protein, and multiple micronutrients in combination have more consistent evidence in deficient groups.
What tests actually help determine whether growth plates are still open?
Bone-age assessment helps determine whether growth potential remains, but it is not the only clue. Signs such as ongoing pubertal progression and tracking on the growth curve also matter. A clinician may use bone age plus growth velocity to decide whether nutrition, hormonal evaluation, or both are needed.
If I look shorter, is it usually my posture or my diet?
Posture can affect apparent height, but it does not replace the biology of growth. If a teenager or adult looks shorter, evaluate posture and spinal health and also check for medical issues affecting height loss, since true height changes may be due to bone density or skeletal conditions rather than diet.
Can working out too much stop someone from growing taller?
Intense training can become harmful if it creates low energy availability, leading to suppressed GH and IGF-1 signaling and compromised bone health (RED-S). The fix is not to avoid exercise, it is to ensure adequate total energy and recovery while matching training load to nutrition.
Will lifting weights stunt a teen’s growth?
Yes, but the key is adequacy and supervision. Structured, age-appropriate resistance training generally does not harm growth plates, while unsupervised excessive loading, poor technique, and chronic under-eating increase risk. Pair training with sufficient protein and overall calories.
Do supplements help if I already eat enough food?
Vitamins and minerals alone cannot “unlock” height if calories are chronically low or if protein is insufficient. If you are supplementing, do it to correct a likely deficiency, ideally guided by symptoms, diet review, and (when needed) bloodwork.
Next Article
If I Quit Smoking, Will I Grow Taller? What to Expect
Does quitting smoking make you taller? Learn growth effects, what changes are possible, timelines, and practical next st