Pregnancy does not make you permanently taller. Your growth plates closed after puberty, and nothing that happens during pregnancy reopens them or adds length to your bones. If you are asking whether there is any way to change your genes to grow taller, the answer is also no, because adult height is limited by growth plate closure can you change your genes to grow taller. What does happen is that pregnancy reshapes your posture, shifts fluid around your spine, loosens your ligaments, and changes the curves in your back in ways that can make your measured height go up or down by roughly a centimeter or so depending on the day, the trimester, and how you're standing. That's not growth. It's biology doing its job to accommodate a growing baby, and most of it reverses after delivery.
Can You Grow Taller During Pregnancy? What’s Real


Why your height might measure differently during pregnancy

If a clinic measurement tells you that you're slightly taller or shorter than you were before pregnancy, there are a handful of real physiological explanations, and none of them involve new bone growth.
Relaxin and ligament laxity
Relaxin is a hormone your body ramps up during the first trimester, and its job is to loosen the ligaments and joints in your pelvis to prepare for birth. The catch is that it doesn't just target your pelvis. Your spine and the rest of your musculoskeletal system feel it too. Cleveland Clinic explains that relaxin can negatively affect posture because the back and pelvis become looser, which shifts how you hold yourself. Relaxin stays in your system well past the first trimester, so this ligament laxity is a sustained feature of pregnancy, not a brief phase. That loosening can subtly change how tall you stand, in either direction.
Spinal curves and posture shifts
Several studies tracking spinal posture through pregnancy have found real, measurable changes in thoracic kyphosis (the upper-back curve) and lumbar lordosis (the lower-back curve). A rasterstereographic pilot study found that thoracic kyphosis increased significantly over the course of pregnancy. Another study in 59 women found that both lordosis and kyphosis increased significantly, and those curves were still present around two months postnatally. A broader PLOS One scoping review noted considerable individual variability: some women showed decreased lumbar curvature in the second trimester while others increased their lordosis by the third. In practical terms, exaggerated spinal curves can compress measured height slightly, just as standing up straight after slouching adds back that same centimeter. National Academies measurement guidance puts the posture-related measurement difference at roughly 1 cm (about 0.4 inches), which is consistent with what you'd see in clinic-to-clinic variation.
Disc fluid and diurnal variation
Your intervertebral discs absorb and release fluid throughout the day. Research on diurnal disc changes in healthy adults has measured stadiometer height variation of about 19 mm on average just from loading and rehydration cycles across a single day. Pregnancy's fluid shifts and the extra load on the spine interact with this normal mechanism, which means your measured height can look slightly different depending on when in the day it's taken and how your discs are loaded at that moment. Again, this is not permanent bone growth.
Swelling (edema)

Fluid retention is common in pregnancy and can affect the legs, feet, and hands. In rare cases it can reach tissue around the spine or contribute to a general sense of bloating and physical change. Mild edema alone isn't a height measurement factor in any meaningful sense, but it is worth noting as part of the broader picture of why your body feels and measures differently during these nine months.
Why actual bone growth doesn't happen in adult pregnancy
Height growth requires active growth plates, the cartilage zones near the ends of your long bones where new bone tissue is laid down during childhood and adolescence. Estrogen plays a direct role in closing those plates during late puberty. Once estrogen signaling triggers growth plate senescence, longitudinal bone growth stops. That process is essentially irreversible: clinical and mechanistic reviews confirm that no nutrition protocol, supplement, or hormonal change in adulthood (including the hormonal cascade of pregnancy) reopens closed growth plates or restarts longitudinal bone growth. Pregnancy delivers a surge of estrogen and other hormones, but those hormones do not reverse growth plate closure. They do plenty of other remarkable things, including remodeling ligaments, shifting calcium metabolism, and altering spinal loading, but growing your skeleton taller is not on that list.
This is worth stating clearly because the same logic applies to questions about whether nutrition or exercise can make an adult taller. If you're wondering about whether nutrition or exercise can make an adult taller, that question overlaps with whether you can "can you make yourself grow taller" during pregnancy. Once the plates are closed, which typically happens in the late teens, the mechanisms for adding bone length simply aren't active anymore. Pregnancy doesn't change that physiology.
Practical ways to look and feel taller during pregnancy

Even though you can't add permanent height, you can absolutely manage posture changes so you're standing at your full actual height rather than an inch shorter because of spinal curve shifts. This matters both for how you look and how much back pain you deal with over the nine months.
Posture and body mechanics
Cleveland Clinic's pregnancy posture guidance is direct: train your body to stand, walk, sit, and lie in positions that place the least strain on your back. In practical terms that means imagining a thread pulling the top of your head upward, keeping your shoulders back and relaxed (not rounded forward), and not letting your lower back collapse into an exaggerated arch as your belly grows. When you need to stand for long periods, adjusting your work surface to a comfortable height reduces spinal loading. Shifting your weight regularly and using a low footrest on one foot can also help distribute load.
Core and back support
Pregnancy-safe strength work that targets the muscles supporting your spine and pelvis helps counteract the ligament loosening from relaxin. Mayo Clinic notes that physical activity and posture work are front-line approaches to managing pregnancy-related back pain. Cleveland Clinic also notes that clinicians can tailor safe workout plans to your trimester and baseline fitness. Gentle exercises like pelvic tilts, swimming, and walking maintain the muscular support that holds you upright. Prenatal yoga is particularly useful because it directly works on spinal alignment and body awareness.
Support belts and mobility aids
Maternity support belts or belly bands can offload some of the anterior weight of your abdomen from your lumbar spine, which often means you naturally stand a little straighter. Mayo Clinic recommends discussing support belts with your healthcare provider to find a fit appropriate for your stage of pregnancy. These are not a fix for posture but they do reduce the fatigue that causes you to slump later in the day.
Footwear choices
High heels shift your center of gravity forward and worsen lumbar lordosis, which is exactly the exaggerated arch you're already fighting during pregnancy. Flat shoes or low supportive heels (around 1 to 2 cm) are generally better for maintaining neutral spinal alignment and reducing back strain. Footwear with good arch support also helps manage the foot flattening that relaxin can cause, which indirectly affects how you stand and carry yourself.
Managing swelling
Mild leg and foot swelling is normal, but significant edema can make movement and posture harder to manage. Elevating your feet when resting, avoiding prolonged standing, staying hydrated, and wearing compression stockings (where appropriate and not contraindicated) are standard strategies. Reducing salt intake can also help. The goal here is comfort and function, both of which make it easier to maintain good posture.
What nutrition, sleep, and exercise can (and can't) do
Getting enough calcium, vitamin D, protein, and iron during pregnancy is genuinely important, but it supports the health of your baby's developing skeleton and your own bone density maintenance, not any increase in your height. Research on blank" rel="noopener noreferrer">calcium and vitamin D supplementation shows relevance to children's growth, where plates are still open, but there is no mechanism by which repletion of any nutrient adds centimeters to adult bone length. Think of adequate nutrition in pregnancy as protecting what you have rather than adding to it.
Sleep matters enormously during pregnancy, but again, the benefit is recovery, hormonal regulation, and fetal development rather than height growth. Growth hormone does peak during deep sleep, and in growing children this matters a lot for height. In adults with closed growth plates, it doesn't translate to added bone length. Getting quality sleep during pregnancy still has real value for energy, mood, tissue repair, and managing the physical load of carrying a baby, just not for growing taller.
Exercise during pregnancy maintains muscle mass, supports posture, helps manage weight gain, and reduces back pain risk, all of which contribute to looking and feeling your best. What it doesn't do is stimulate longitudinal bone growth. The 82% back-pain prevalence reported in one pregnancy posture study is a reminder that staying active and maintaining postural strength is genuinely protective, even if the mechanism isn't height gain.
When to check with your clinician
Most posture and measurement changes during pregnancy are normal and explainable. But certain symptoms alongside physical changes warrant prompt evaluation, not next-appointment-level, prompt.
- Sudden or significant increase in swelling in your face, hands, or feet: this can be a sign of preeclampsia, and NHS guidance is to call your midwife, GP, or labour ward immediately. Mayo Clinic echoes that sudden edema, especially in the face and hands, may indicate preeclampsia.
- Back pain that is severe, suddenly worsening, or accompanied by neurological symptoms like leg numbness, weakness, or bladder/bowel changes: these may indicate nerve compression or another structural issue that needs assessment beyond standard pregnancy back pain.
- Noticeable and rapid change in your height measurement or spinal shape at a clinic visit that your provider doesn't explain: while small measurement variations are normal, significant or sudden changes deserve discussion.
- Pelvic pain that is disabling or makes walking, climbing stairs, or turning in bed very difficult: this may be symphysis pubis dysfunction (SPD) or pregnancy-related pelvic girdle pain (PGP), both of which respond to physiotherapy and specific movement strategies but need a proper diagnosis first.
- Any new bone pain, rib pain, or joint swelling that is asymmetric or doesn't fit the usual pattern: while uncommon, these can occasionally signal bone-related conditions worth ruling out.
The bottom line is that if a physical change feels wrong rather than just uncomfortable, get it evaluated. Pregnancy involves a lot of normal discomfort, but it also creates conditions that can mask or mimic more serious issues.
Realistic expectations: what pregnancy actually changes about your body
Your height is essentially set by your genetics and the growth environment of your childhood and adolescence. How tall you grew was shaped by factors like parental height, nutrition during development, sleep quality when your plates were open, and overall health during those years. In the long run, genetics largely determines whether you can grow taller than your parents, and there are no proven adult interventions that reopen growth plates parental height. By the time you are pregnant, that story is largely written. Pregnancy doesn't reopen it. Can you grow taller than your genetic height? For adults, the evidence-based answer is no, because closed growth plates do not restart bone lengthening.
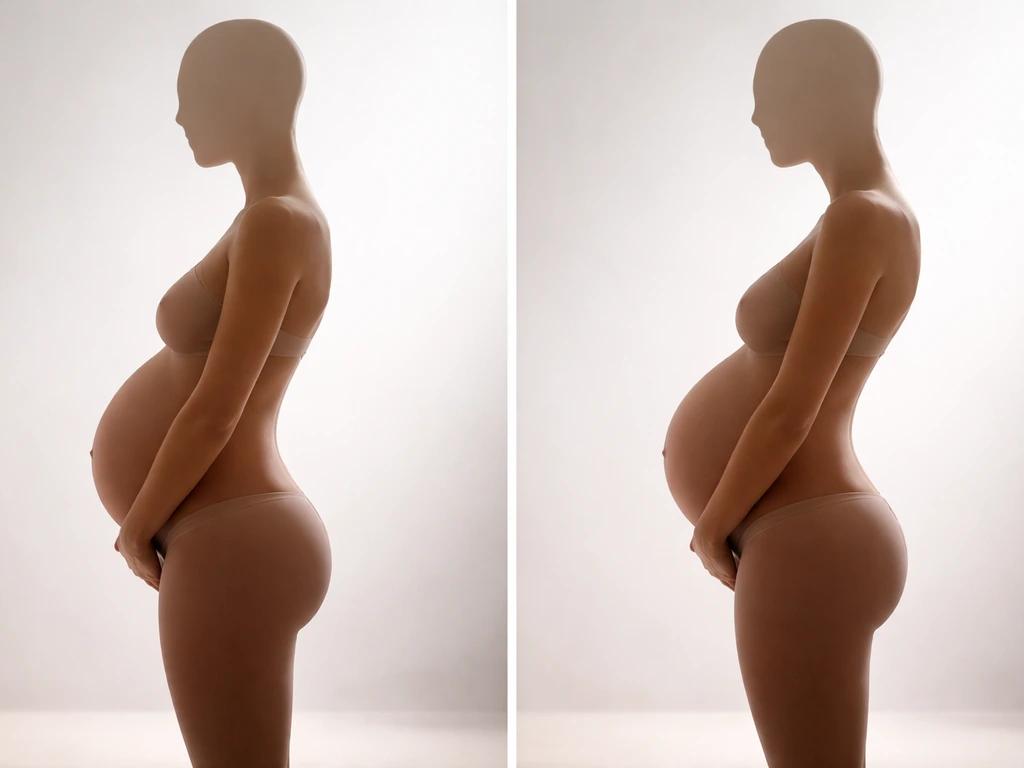
What pregnancy does change, temporarily and sometimes for longer, is your posture, spinal curves, ligament tension, and the functional height you express from your actual skeletal height. A woman who enters pregnancy with good postural habits and maintains them through appropriate exercise and body mechanics awareness will likely come through the experience at the same measured height she started with. Someone who lets pregnancy's physical demands lead to progressive slouching, muscle weakening, and untreated back pain might measure slightly shorter postnatally, at least for a while.
If you're genuinely curious about the broader science of adult height and whether there are any evidence-based levers left after growth plates close, that's a topic worth exploring separately. If you're asking, "is it possible to grow taller" in general, the key issue is whether growth plates can still lengthen your long bones. The short version is that the ceiling is set by genetics, and while posture and disc health can recover or decline by a centimeter or so across a lifetime, no intervention has been shown to add permanent height to an adult skeleton. Managing postural health during pregnancy is worth doing for comfort, pain reduction, and function, and those are legitimate and important goals even without any height benefit attached.
Focus on the practical wins: stand tall, support your core, choose supportive footwear, manage swelling early, and work with your healthcare team on any pain that limits your movement. You won't come out of pregnancy taller, but you can absolutely come out of it with a healthier spine and better postural habits than you went in with.
FAQ
If my height changes during pregnancy, how can I tell whether it’s real or just posture or measurement variation?
Any true increase in height you notice during pregnancy is almost always a measurement or posture change, not bone lengthening. If you want to compare fairly, measure at the same time of day (many people are slightly taller later in the day) with the same device, and stand the same way for several trials.
How long does it take to “go back to normal” after giving birth?
After delivery, ligament looseness and spinal curve changes often improve over weeks to a couple of months, but not everyone fully returns to their pre-pregnancy posture. If you are still having persistent posture-related pain or your measured height continues to drop noticeably, ask your clinician or a pelvic floor or physical therapy specialist to assess alignment and core strength.
Can prenatal exercise help me look taller even if it cannot change bone length?
Prenatal strength training and yoga can improve how well you stack your spine and support your pelvis, which can help you look taller by standing straighter. But if the exercises increase pain, cause numbness, or worsen back symptoms, scale back and get personalized guidance, since pregnancy-safe plans should be tailored to trimester and your baseline fitness.
What are common mistakes that make clinic height readings misleading during pregnancy?
A routine stadiometer or clinic measurement can be thrown off by flexing your hips, slumping shoulders, or standing with weight shifted to one leg. If you suspect a “directional” error (for example, always shorter on one day), repeat measurements on the same side you tend to favor, and consider having a clinician repeat the measurement with standardized posture cues.
Are maternity support belts likely to make me taller, and are there any safety cautions?
Support belts and belly bands can reduce how much your abdomen’s weight pulls your spine forward, which may reduce slumping and make you feel more upright. However, they are not meant to replace posture mechanics or exercises, and you should stop and get advice if the band causes numbness, skin irritation, or worsening discomfort.
What symptoms would mean I should not assume my height change is just normal posture in pregnancy?
If you have severe back pain, a noticeable change in posture, or new neurological symptoms (like leg weakness, tingling, or radiating pain), that is not something to treat as “just posture.” Get prompt evaluation, because pregnancy can unmask spine, pelvic, or nerve issues that need targeted care.
Should I take any supplements or follow a diet plan specifically to gain height during pregnancy?
Most nutrients in pregnancy support fetal development and maternal maintenance, they do not reopen growth plates or add adult bone length. Prioritize adequate protein and minerals for tissue health, but avoid high-dose supplements for “height” goals, since excess iron, vitamin A, or other nutrients can be harmful.
Why might my height seem different depending on the time of day, and how should I track it?
Diurnal disc and fluid shifts mean your measurement can vary within the same day, often by enough to matter on a clinic scale. If you are tracking changes, measure in the morning after using the bathroom and before long periods of standing, or do consistent morning vs evening comparisons.
What practical changes help me maintain my full functional height as my belly grows?
Even with posture improvements, you may feel shorter because of balance changes and how you carry your body as the belly grows. If you want functional “taller” results, focus on neutral spine cues, supportive footwear, and keeping glutes and core engaged during standing and walking, rather than trying to force an exaggerated arch.
Can You Grow Taller Than Your Genetic Height? Facts
See if you can exceed genetic height, what controls growth plates and puberty, and how to maximize or adjust height safe