You cannot grow taller than your genetic ceiling once your growth plates have fused, which typically happens near the end of puberty. That is the honest answer. But here is the nuance most people miss: genetics sets a range, not a fixed number, and many people never actually reach the top of that range because of preventable factors like poor nutrition, inadequate sleep, or untreated health conditions. So if you are still growing, the real question is not whether you can beat your genes, but whether you can reach the full height your genes already allow. If you are an adult, the question shifts to something different entirely, and there are still realistic options worth understanding.
Can You Grow Taller Than Your Genetic Height? Facts

Marcus Reeves
14 May 2026
What your genetic height actually means
Height is polygenic, meaning it is influenced by hundreds of genetic variants, not a single gene. Your parents' heights give a useful rough estimate of where you might land, but the prediction range is wider than most people expect. The American Academy of Pediatrics emphasizes that the mid-parental method is a rough estimate and that using growth charts and growth trajectory helps predict adult height. The standard mid-parental height method works like this: add both biological parents' heights together, adjust by adding 2.5 inches (about 6.5 cm) if you are male or subtracting 2.5 inches if you are female, then divide by two. That number is your mid-parental target. But the American Academy of Pediatrics notes that 95% of children end up within about 4 inches (roughly 10 cm) above or below that target. Some pediatric frameworks put the expected range at plus or minus about 8.5 cm around the mid-parental estimate. Either way, there is real spread. Two siblings with the same parents can differ meaningfully in adult height.
What this means practically is that your genetic blueprint gives you a range, not a destiny. The top of that range is what most people are hoping to hit when they ask whether they can grow taller than their genetic height. Whether you can grow taller than your parents is largely about whether your growth plates are still open and whether you are maximizing the factors that influence your genetic range whether you can grow taller than your genetic height. You probably cannot exceed the ceiling, but you can absolutely fall short of it, and that gap is where lifestyle and health factors genuinely matter. Whether you can change your genes to directly alter height is a separate question, and current science gives that idea very little support. Some adults still look for answers to whether you can change your genes to grow taller, but the main levers are different change your genes to directly alter height.
When height growth is actually possible
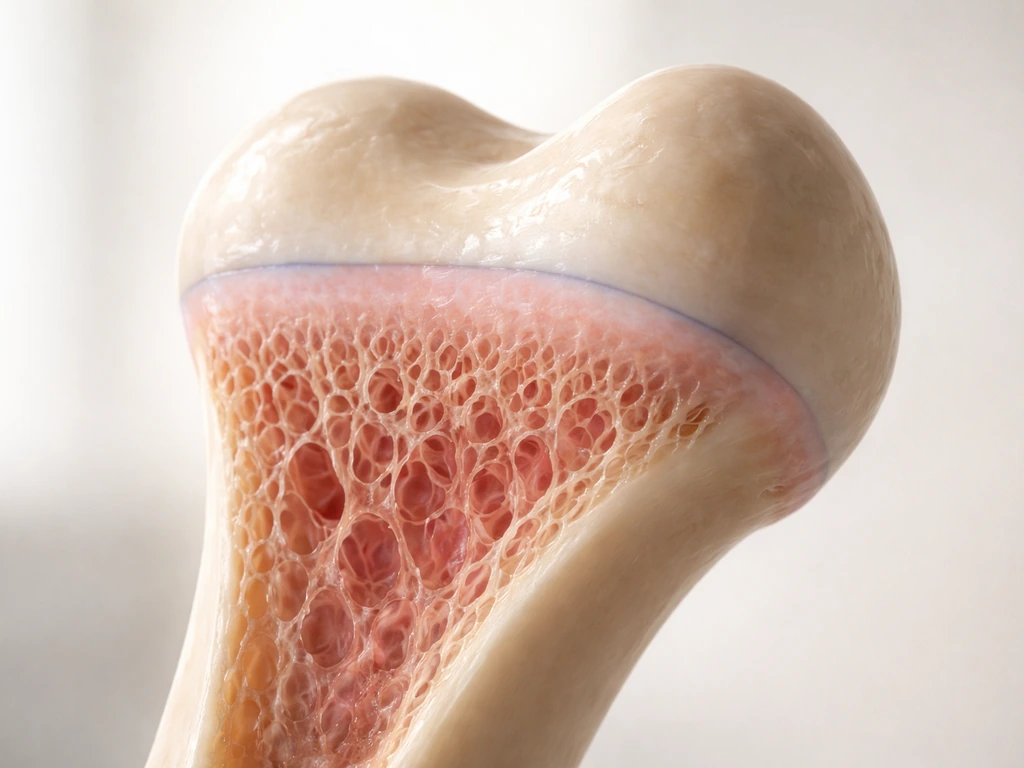
Linear height comes from your long bones getting longer, and that happens at the growth plates, which are soft cartilage zones near the ends of bones like your femur and tibia. As long as those plates stay open, bone can keep growing. Once they fuse, longitudinal growth from those sites is done. Duke Health notes that different bones stop growing at different times, making the exact closure date hard to predict, but the overall pattern is consistent: growth plates close near the end stages of puberty. Rady Children's Hospital describes the same window, emphasizing that once closure happens, long-bone growth potential ends.
For most people, that means the active growth window runs through the teenage years. Girls typically finish growing a couple of years after their first period, often by their mid-teens, while boys tend to grow into their late teens, sometimes even seeing small gains into their early twenties. Puberty timing varies significantly between individuals, which is why some 16-year-olds are already done growing while others still have a few inches to add. If you are a teenager and puberty seems delayed compared to peers, that detail matters a lot, and it is worth discussing with a doctor.
Levers you can actually pull during your growth window
If your growth plates are still open, these are the factors that genuinely influence whether you reach the upper end of your genetic range. None of them are magic, but each has real physiological backing.
Nutrition: calories and the right building blocks

Chronic undernutrition is one of the most consistent limiters of height potential in children and adolescents. Your body needs enough total calories to fund growth, and it needs adequate protein because bone and muscle building require amino acids. Beyond macros, specific micronutrients are closely tied to skeletal development. Calcium and vitamin D are the obvious ones since they directly support bone mineralization. Zinc matters too because it plays a role in growth hormone signaling and cell division. Iron deficiency, which is common in adolescents, can blunt growth indirectly by causing fatigue and reducing the quality of nutrition overall. The practical take: eat enough, prioritize protein at each meal, include dairy or fortified alternatives for calcium, get reasonable sun exposure or supplement vitamin D if you live somewhere overcast, and eat varied whole foods rather than relying on processed options.
Sleep: where a lot of the actual growing happens
Growth hormone is released primarily during deep sleep, which makes sleep quality and quantity genuinely important during the growth years, not just good advice for productivity. Teenagers need 8 to 10 hours per night according to most pediatric guidelines, and many are getting considerably less. Chronic short sleep can suppress growth hormone output. This is one of the more concrete mechanisms linking a lifestyle factor to linear growth, not just a general wellness claim.
Managing chronic illness and stress
Uncontrolled chronic conditions, whether gastrointestinal diseases that limit nutrient absorption, asthma managed poorly, or anything else that keeps the body in a sustained stress state, can redirect resources away from growth. Chronically elevated cortisol in particular is known to suppress growth hormone. Getting chronic conditions properly treated is not a marginal detail; it can make a real difference in final height for affected kids.
Exercise and posture: what actually helps

Here is where a lot of myths live. No exercise makes your bones longer directly. You cannot stretch your femur by hanging from a bar. Resistance training done appropriately does not stunt growth in children or adolescents, which is a persistent worry that the research does not support when loads are age-appropriate and form is correct. What exercise does do during the growth years is support overall health, promote good sleep, and may encourage healthy growth hormone signaling as part of a generally active lifestyle. That is genuinely useful, just not the direct bone-lengthening effect some people imagine.
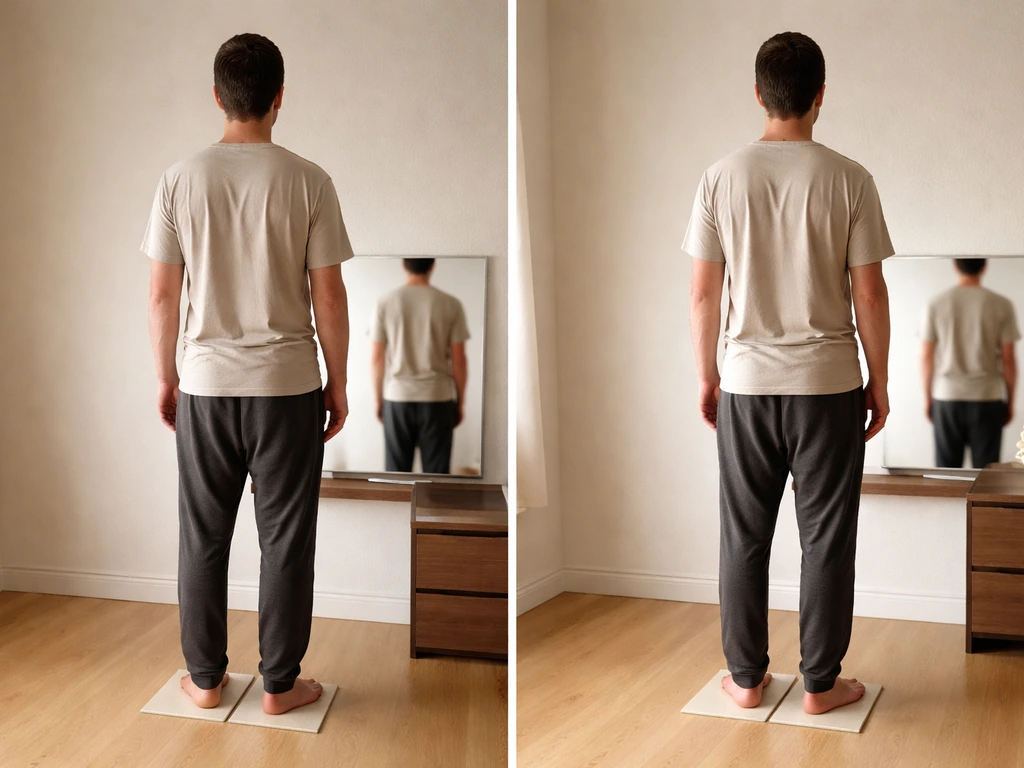
Posture is a different story and worth separating out. Habitual poor posture, particularly thoracic kyphosis from slouching at screens, can make you look shorter than you are by compressing spinal curves. Strengthening the posterior chain (back extensors, glutes, scapular stabilizers) and improving hip flexor flexibility can meaningfully improve standing height appearance. This is not making you taller in the bone-length sense, but for some people, fixing posture reveals an inch or more of height they already had.
Medical options if you are still growing
If a child or teenager is growing significantly slower than expected, or if their height trajectory is falling away from their predicted range, that warrants medical evaluation rather than a wait-and-see approach. A pediatric endocrinologist can assess whether growth hormone deficiency, hypothyroidism, Turner syndrome, or other endocrine conditions are involved. Delayed puberty is another scenario where evaluation matters: constitutional delay (simply a late bloomer) is common and usually resolves on its own, but secondary causes like nutritional deficiency or chronic illness need to be identified and addressed.
Recombinant growth hormone therapy is an established treatment for children diagnosed with growth hormone deficiency and certain other conditions like Turner syndrome or short stature homeobox gene deficiency. It is FDA-approved for those specific indications. It is not a general-purpose height enhancer, and prescribing it outside approved conditions is not standard practice. If a child is consistently below the third percentile on growth charts, deviating significantly from their mid-parental height expectation, or showing no pubertal development by expected ages, those are the flags that prompt a proper workup.
Can adults actually grow taller
Once growth plates have fused, true longitudinal bone growth is not happening through lifestyle changes. That is simply the biology. However, there are a few things worth knowing for adults who care about their effective standing height.
Spinal decompression effects are real but temporary. After a night of sleep, intervertebral discs rehydrate and you are measurably taller in the morning than after a full day of being upright under gravitational load. This difference can be around 1 cm or slightly more. It does not represent a true height gain; it reverses within hours. Sustained improvements in spinal loading habits and core strength can help maintain the taller end of this daily range more consistently, but the gain is modest.
Posture correction, as mentioned, is the most accessible and evidence-supported route to appearing and measuring taller as an adult. A person with significant thoracic kyphosis who improves their posture through targeted exercise and awareness can see meaningful differences in how tall they stand and measure. This is not cosmetic illusion; it is your actual height measured more accurately.
Limb lengthening surgery exists and is performed by orthopedic surgeons for adults with significant short stature or limb length discrepancies. The procedure involves controlled bone fracture, gradual distraction to encourage new bone formation, and a lengthy recovery period. It can add meaningful height, typically 2 to 3 inches per treatment course. However, the risks are substantial: infection, nerve damage, joint complications, and a recovery that spans many months. It is not a casual elective procedure, and reputable providers reserve it for appropriate clinical situations. Weight management also matters indirectly: excess body weight can worsen posture and joint loading, while being at a healthy weight allows you to stand and move in a way that represents your full height more accurately.
How to figure out where you actually stand
If you are a parent tracking a child's growth, or a teenager trying to gauge your own potential, the most practical step is to plot height measurements on a standardized growth chart every 6 to 12 months. What matters most is not a single measurement but the trajectory over time. A child consistently tracking along the 40th percentile is growing normally; a child whose percentile has been dropping over several measurements is showing a pattern worth investigating.
Calculate the mid-parental height target using the method above and use it as a rough reference, not a hard number. If measured growth trajectory points well below that target range, or if growth seems to have stalled unexpectedly, that is the time to bring in a pediatric provider. Bone age X-rays (typically of the wrist) can give a clearer picture of how much growth potential remains by showing how far the growth plates have progressed toward fusion.
Red flags that warrant a doctor visit
- Height consistently below the 3rd percentile on standardized growth charts
- Growth rate that drops across two or more major percentile lines over time
- No signs of puberty by age 14 in boys or age 13 in girls
- Significant discrepancy between child's height and mid-parental height target (more than 8 to 10 cm below)
- Unexplained weight loss, fatigue, or other symptoms alongside slow growth
- A teenager who has not grown at all in the past year and is not close to the expected end of puberty
The bottom line is this: genetics sets the range, but it does not guarantee you hit the top of it. If you are still in your growth window, the most impactful things you can do are unglamorous but real: eat enough of the right foods, sleep adequately, manage any chronic health issues, and stay active. If you are still growing, focusing on sleep, nutrition, and managing any health issues can help you reach the upper end of your genetic range growth window. If something seems off about a child's growth trajectory, get it evaluated sooner rather than later because the window to act is time-limited. And if you are an adult asking whether you can grow taller than your genetic height, the honest answer is no for bone length, but yes for the height you actually express through posture, body composition, and spinal health. That distinction matters more than most people realize. But pregnancy is a different situation because most people are already past their active growth window by then.
FAQ
If my parents were short, can I still grow taller than them? (Or will I always fall short?)
Yes, but the timing matters. If you are still in puberty and your growth plates are not fused, better nutrition, sleep, and medical management can help you reach the upper end of your genetic range. If you are fully mature or growth plates have fused, you cannot add bone length, and changes will mainly come from posture, core strength, and body composition rather than true height growth.
How do I tell if I am actually growing or if the measurement is just off?
Single height measurements are misleading. Use a consistent method (same time of day, similar clothing, back against a wall) and track a series of readings. A pattern like dropping percentiles or slowing velocity for 6 to 12 months is more informative than one “bad” number.
What if I sleep, but my bedtime is inconsistent or I get fewer than 8 hours?
Sleep quantity is more important than sleep “quality” alone. If you are getting far less than 8 to 10 hours nightly, growth hormone release can be blunted during your growth years. Also avoid chronic late-night sleep schedules, because a consistently shifted bedtime can reduce effective sleep time.
Do vitamin D or calcium supplements reliably make you taller?
It can matter indirectly. Calcium, vitamin D, protein, and overall calories support bone building, but using one supplement without correcting overall diet often does not move the needle. If you suspect deficiency, it is usually more useful to adjust food intake and, when appropriate, ask a clinician about labs rather than taking high-dose supplements blindly.
Can dieting or eating less to lose weight stunt growth?
Occasionally. Very large calorie restriction, low protein intake, or eating disorders can suppress growth and delay puberty. “Normal” dieting behavior can still affect height if it chronically reduces calories or removes key nutrients required for growth.
If I have a stomach or autoimmune condition, does it affect my height potential?
Poorly managed chronic inflammation or hormone problems can. Examples include celiac disease, inflammatory bowel disease, poorly controlled asthma, and thyroid disorders, which can reduce nutrient absorption or alter growth signaling. If growth is slower than expected, addressing underlying conditions is usually higher impact than trying to “optimize” supplements.
Can weightlifting stunt growth, or is it safe for teens who want to maximize height?
It depends on what you mean by “height.” Resistance training itself does not stunt growth when done with age-appropriate loads and safe technique. However, extremely high training volume combined with low calories or poor recovery can contribute to fatigue and reduce your ability to support growth.
Why do I seem taller some days and shorter others, even though my bones are not changing?
Sometimes, and it is a common source of confusion. If you are measuring at different times of day, your standing height can vary due to spinal disc hydration and posture. For comparisons, measure in the morning close to the same time each day or use average values rather than a single morning or evening number.
What posture changes actually help you measure taller, and what is just a myth?
Yes, and the target is “upper body position” and mechanics, not stretching your legs. Focus on thoracic posture and spinal alignment, plus strengthening back and hip muscles. If you have structural spinal issues or significant pain, get evaluated before aggressive stretching routines.
Is growth hormone therapy something everyone should consider if they want to be taller?
If you are diagnosed with growth hormone deficiency or certain genetic conditions, treatment can be appropriate. But growth hormone is not recommended as a general height booster, and dosing should be individualized with monitoring. A clinician will also consider other causes such as thyroid problems or delayed puberty before starting therapy.
If my puberty started late, does that mean I will automatically get taller?
Likely yes if growth plates are still open, because delayed puberty can mean more time before closure. But delayed timing can also reflect treatable causes like nutritional deficiency or chronic illness. The key is whether it is constitutional delay versus a secondary medical issue, which requires clinical assessment.
Does being overweight reduce your actual height, or is it only posture?
Body weight can affect apparent height through posture and spinal loading, especially in people carrying extra abdominal weight that increases slouching. Weight loss that improves posture can increase measured standing height modestly, but it will not create new bone length once growth plates are closed.
Can you grow taller during pregnancy?
Pregnancy is generally separate because most people are not growing through bone length during pregnancy, and height changes are usually due to posture, muscle tone, and spinal disc loading. So the “can I grow taller?” question during pregnancy should not be treated like a growth plates scenario.
Next Article
Can You Make Yourself Grow Taller? What Works and What Does Not
Can you make yourself grow taller? Evidence on genetics, growth plates, sleep, nutrition, and safe medical options by ag
