Losing weight won't make your bones longer, but it's not a completely useless question either. For kids and teenagers who still have open growth plates, carrying excess body fat can interfere with the hormonal environment that drives growth, and bringing weight into a healthier range may help that process work better. For adults, whose growth plates have long since fused, weight loss won't add a single millimeter of true bone-length height, though you might look and measure slightly taller due to changes in posture and spinal compression. If you're wondering whether excess weight affects your final height, the key is your growth stage, especially whether growth plates are still open. The honest answer depends almost entirely on your age and whether you're still growing.
Does Losing Weight Help You Grow Taller? Evidence-Based Guide


True height vs. "apparent" height: why the difference matters
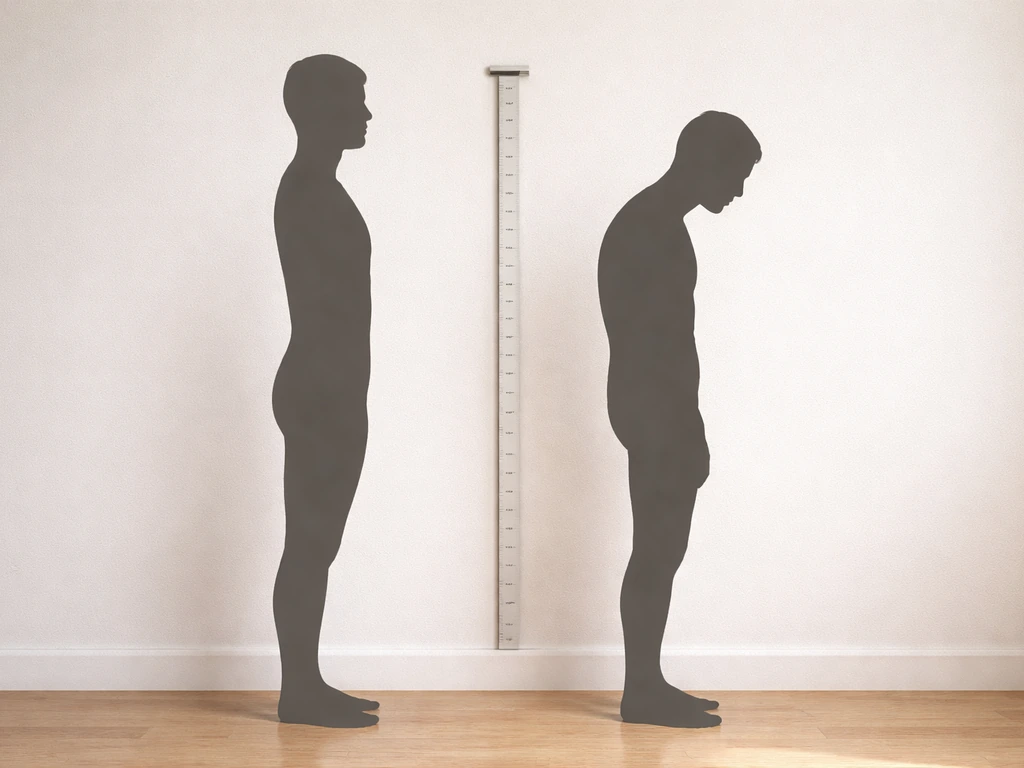
Height has two components that often get conflated. True height is determined by bone length, particularly the long bones of the legs and the stacked vertebrae of the spine. The amount on a scale does not increase your true bone length, but weight can affect what a tape measure shows True height. That only increases when growth plates (the cartilage zones at the ends of long bones) are still open and actively laying down new bone tissue. Apparent height is what a tape measure or stadiometer records on any given day, and it can shift without any change in bone length at all.
Spinal compression is a real and measurable phenomenon. Research using MRI and stadiometry shows that disc height and spinal length change throughout the day based on loading, posture, and body weight. When you carry excess weight, you compress the intervertebral discs more, which can shave off a measurable amount of standing height. Lose that weight, decompress the spine, and stand up straighter, and you may genuinely measure a little taller, without a single growth plate being involved. The same principle applies to posture: slouching redistributes spinal load and reduces measured height, while improved posture from better core strength and reduced anterior pelvic tilt can add a centimeter or two to your stadiometer reading. These are real changes you can see and feel, but they are not the same as growing taller. This is not about pushing the earth down, because standing height depends on bone length and how much your spine compresses and decompresses over the day push the earth down when you grow taller. Back pain when you grow taller is often linked to spinal compression, posture changes, and normal musculoskeletal strain rather than actual bone lengthening.
How excess body fat can affect growth in kids and teens
This is where the biology gets genuinely interesting, and where the answer is more nuanced than a flat no. Obesity in childhood alters several hormonal systems that are deeply tied to growth.
The leptin and puberty connection
Leptin is a hormone produced by fat cells, and blank" rel="noopener noreferrer">higher body fat means higher leptin levels. Leptin acts as a signal of energy sufficiency to the brain, including the hypothalamus regions that govern puberty. Research consistently shows that blank" rel="noopener noreferrer">elevated leptin from excess adiposity can push puberty to begin earlier than it otherwise would. That sounds harmless, but earlier puberty means the growth plates are exposed to sex hormones sooner, which accelerates their fusion. The net result is a shorter growth window, and children who go through puberty early often end up at a lower final adult height than they might have reached with a later pubertal timeline. A large Swedish longitudinal study confirmed this pattern: overnutrition in early childhood temporarily boosts childhood height gains, but earlier pubertal maturity and compressed adolescent growth compensate for it, ultimately not benefiting final height.
IGF-1, insulin, and the growth hormone axis
Obesity also disrupts the growth hormone/IGF-1 axis. Obese children tend to have altered IGF-1 binding protein patterns and elevated insulin levels that can blunt the normal growth-promoting signaling cascade. Studies on obese children undergoing lifestyle-based weight loss interventions have found that these hormonal alterations are largely reversible: after weight reduction, leptin, insulin, and IGFBP-3 patterns normalize. Crucially, the same research found that weight loss through lifestyle intervention was not associated with any disturbance to linear growth, meaning the kids didn't lose height velocity as a result of losing weight.
Sleep quality and growth hormone release

Growth hormone is predominantly secreted during deep sleep, particularly in slow-wave sleep stages. Excess weight, especially around the neck and throat, dramatically increases the risk of obstructive sleep apnea and fragmented sleep architecture. When sleep is disrupted, growth hormone pulses are blunted. For a growing child or teenager, that's a meaningful physiological cost. Improving weight in this context doesn't just feel better, it can restore the sleep quality that underpins normal growth hormone secretion.
Age is everything: growth plates close and that's that
The single most important variable in this whole discussion is age relative to skeletal maturity. Growth plates (epiphyseal plates) typically fuse in late adolescence, generally between ages 14 and 19 in girls and 16 to 21 in boys, though there's real individual variation. Once fused, they cannot be reopened by any intervention, including weight loss, nutrition changes, stretching, or anything else. A bone density scan or hand/wrist X-ray can show whether growth plates remain open, which is why pediatric endocrinologists often order these when evaluating growth concerns.
| Age group | Growth plates | Can weight loss affect true height? | What it can realistically do |
|---|---|---|---|
| Young children (2–10) | Open | Possibly, by supporting healthier hormonal environment | Reduce risk of early puberty, support better sleep/GH release |
| Teenagers (11–18) | Open but closing | Potentially, especially early in puberty | Normalize IGF-1/leptin, protect remaining growth window |
| Young adults (18–21) | Closing or recently fused | Unlikely for true height; unclear window | Improve posture, reduce spinal compression |
| Adults (21+) | Fused | No effect on bone length | Improve posture, reduce spinal compression, better health overall |
What weight loss can and can't realistically do
Let's be direct about the ceiling here, because this topic attracts a lot of wishful thinking.
- Weight loss cannot reopen fused growth plates. There is no biological mechanism for this, in adults or anyone else.
- Weight loss cannot make bones longer after skeletal maturity. Bone remodeling continues throughout life, but it doesn't add length.
- Weight loss will not guarantee extra centimeters of height even in growing children. It may support a healthier growth environment, but genetics set the ceiling.
- Weight loss can reduce spinal compression and improve posture, which may add 1 to 2 centimeters of measured height without changing any bone.
- In children and teenagers with obesity, achieving a healthier weight may help normalize the hormonal disruptions that could otherwise shorten the growth window, but the evidence doesn't promise a specific height gain.
- Extreme caloric restriction during childhood or adolescence can actively harm growth by depriving the body of the raw materials (protein, calcium, zinc, vitamin D) needed to build bone.
A prospective cohort study tracking height and growth velocity in children and adolescents undergoing obesity treatment found that large cohort data generally show no significant difference in final height between individuals with obesity and those of normal weight. The bigger risks of untreated childhood obesity on height relate to puberty timing rather than a direct suppression of growth hormone. This is a subtle but important distinction.
How to approach weight management safely if growth is a concern
If you're a parent of a child with overweight or obesity, or a teenager navigating this yourself, the goal is never aggressive weight loss. The Endocrine Society's pediatric obesity guidelines are clear: the focus should be on healthy lifestyle behaviors, not rapid weight reduction. Extreme calorie restriction (very-low-calorie diets) is explicitly not recommended for growing children because of the risk of nutrient deficiencies that directly impair bone development.
Practical targets that support healthy weight and growth
- Aim for at least 60 minutes of moderate-to-vigorous physical activity daily. The Endocrine Society recommends starting with a minimum of 20 minutes and building toward 60. Weight-bearing exercise also stimulates bone density and supports the musculoskeletal system.
- Prioritize protein, calcium, and vitamin D. These are non-negotiable for bone-building during growth. Cutting calories by eliminating dairy, meat, or legumes is counterproductive.
- Don't chase rapid weight loss. In children, the goal is often weight maintenance while height increases (effectively reducing BMI over time), not an aggressive drop on the scale.
- Protect sleep. Aim for 9 to 11 hours for school-age children and 8 to 10 hours for teenagers. Consistent, high-quality sleep is when the bulk of growth hormone is released.
- Reduce ultra-processed food and sugar-sweetened beverages. These drive caloric excess and insulin spikes without delivering the micronutrients growth requires.
- Involve a registered dietitian or pediatric specialist. Caloric targets during growth phases need to be individualized, not pulled from adult weight-loss frameworks.
A note on posture-focused strategies for adults
For adults who have asked this question hoping for a true height boost, the honest play is to optimize apparent height. Core strengthening exercises (planks, dead bugs, bird dogs), reducing anterior pelvic tilt, and addressing thoracic kyphosis through mobility work can genuinely improve standing posture and measurement. Carrying less abdominal weight also reduces the forward pull on the lumbar spine, which contributes to a taller, more upright stance. None of this grows bone, but it's real and worth pursuing for health and confidence reasons alike.
When to see a doctor and how to evaluate your growth potential
If a child or teenager is significantly shorter than peers, or if growth seems to have stalled, that warrants a conversation with a pediatrician sooner rather than later. The Endocrine Society is clear that the goal of medical evaluation is to determine whether growth concerns reflect a treatable medical condition (like growth hormone deficiency, hypothyroidism, or celiac disease affecting absorption) versus normal variation.
Some specific red flags that should prompt a doctor visit include a linear growth velocity below 4 centimeters per year in a school-age child, no signs of puberty by age 13 in girls or age 14 in boys, or a significant height gap between a child and their calculated mid-parental height target. These aren't panic signals, they're just thresholds where a clinician can actually look at bone age, run hormone panels, and give real data rather than guesswork.
What a doctor will actually assess

- Bone age X-ray (typically of the left hand and wrist) to determine skeletal maturity versus chronological age
- Growth velocity calculated from height measurements taken at least 6 months apart
- IGF-1 and IGFBP-3 levels to assess the growth hormone axis
- Thyroid function, complete blood count, and metabolic panel to rule out systemic causes
- Pubertal staging to assess where a child is in the Tanner scale
- Mid-parental height calculation to set a realistic genetic target
The factors with the strongest evidence for supporting height potential during growth are genetics (by far the largest driver), adequate overall caloric intake with high nutrient density, consistent high-quality sleep, regular physical activity including weight-bearing exercise, and normal hormonal function. Weight management matters insofar as it supports those underlying factors, not as a height hack in its own right. If you've been wondering whether being skinny versus carrying more weight influences height independently, that question has its own nuances worth understanding separately. It can help to understand how body fat affects growth mainly through things like growth plates and hormone timing, rather than through extra height from weight alone being skinny versus carrying more weight influences height independently.
The bottom line is straightforward: lose weight if it serves your health, and if you're a growing child or teen with obesity, doing so safely and gradually may help your body's growth systems function closer to their potential. But frame it as supporting the process, not triggering it. Height is largely determined by genetics and the quality of the environment during your growth years, and no scale number changes that fundamental biology.
FAQ
If I lose weight as an adult, can my growth plates ever reopen and let me grow taller for real?
No. Once epiphyseal (growth) plates fuse, they cannot reopen due to weight loss, stretching, or diet changes. What you might notice after losing weight is higher apparent height from less spinal compression and better posture, not new bone lengthening.
Why do two people with the same bone length measure different heights at different times of day?
Because standing height is affected by daily spinal loading, disc compression, and posture. Even without any change in bone length, measurement can vary based on how your spine is stacked that day (for example, after long sitting versus standing, or after exercise).
Can rapid or extreme dieting in a teen cause height problems?
Yes. Very low-calorie or aggressive calorie restriction can reduce nutrient availability needed for growth and can worsen sleep or energy balance. The goal for teens is safer lifestyle-based changes that support growth and bone development rather than quick weight drops.
Does exercise help with height measurements the same way weight loss does?
Exercise can improve apparent height by strengthening the core and improving posture (which reduces forward pelvic tilt and slouch). But it will not increase true bone length once growth plates are closed, so the benefit is measurement and mechanics, not taller bones.
If my child’s puberty starts early, will weight loss delay puberty and improve final height?
Weight reduction in childhood can help normalize some hormone signals, but early puberty can also be driven by genetics and other factors. If puberty starts early, the most practical next step is evaluation by a pediatrician or pediatric endocrinologist, because timing and potential treatments depend on the cause, growth velocity, and bone age.
Is it possible for a child with obesity to be taller during childhood but end up shorter as an adult?
Yes. Early childhood weight-related hormonal changes can be associated with earlier puberty, and earlier puberty shortens the overall growth window. That can mean more height gain early on, then less total final height later compared with peers who go through puberty later.
How can we tell whether a growth concern is normal variation versus a medical issue?
Track growth velocity over time (height change per year) and compare it with standardized charts and target height based on family history. If growth slows, puberty is absent when expected, or there is a large gap from mid-parental height, clinicians can use bone age and possibly lab tests to sort out treatable causes.
What measurement mistakes make parents think weight loss made their child taller?
Common errors include measuring at different times of day, using inconsistent posture (slouched versus upright), not using a proper stadiometer, and comparing without noting footwear or hair position. If you remeasure, do it under the same conditions, ideally at similar times and with consistent technique.
Do bone density scans or hand-wrist X-rays always show whether my child can still grow?
They can be used to estimate skeletal or bone age and whether growth plates are still open, but interpretation requires a clinician. A pediatric endocrinologist typically combines imaging with growth history and, when indicated, labs to judge remaining growth potential.
What is the most helpful goal for height if I am an adult or my child is near skeletal maturity?
Focus on apparent height and spine health. For adults, core and mobility work, plus reducing excess abdominal load, can improve upright posture and stadiometer readings. For teens nearing maturity, the priority is healthy growth support (sleep, nutrition, activity) and identifying any medical reasons for slowed growth rather than trying to “hack” height.
Do You Gain Weight When You Grow Taller? Science Answers
See if weight gain makes you taller, how growth plates and puberty work, and which nutrition habits support height.
