Limb-lengthening surgery can add real, measurable height, but it comes with a complication rate that most people searching this topic are not prepared for. Even with modern internal nail devices, studies report per-segment complication rates ranging from roughly 31% to 46% depending on the device used. Pain, muscle tightness, nerve irritation, joint stiffness, and the very real possibility of a revision surgery are not rare edge cases. They are common enough that every credible orthopedic center frames this as a major, months-long procedure, not a shortcut. Before getting into exactly what can go wrong, it helps to understand what the surgery actually is and who is genuinely a candidate.
Surgery to Grow Taller Side Effects, Risks, and Recovery

Marcus Reeves
2 Jul 2026

What 'height surgery' actually means
When people search for surgery to grow taller, they almost always end up reading about limb-lengthening procedures, specifically distraction osteogenesis applied to the femur (thigh bone) or tibia (shin bone). The core idea is the same regardless of which device is used: the surgeon cuts the bone, then very slowly separates the two segments so that new bone fills the gap. That new bone, called the regenerate, is what produces the height increase.
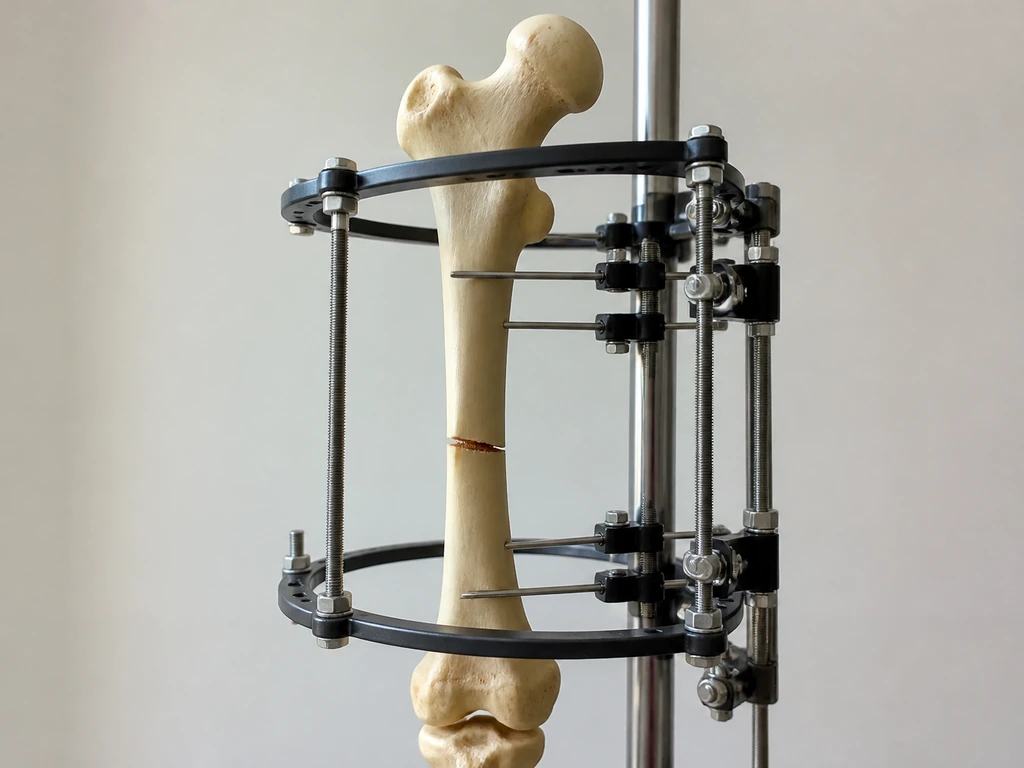
There are two main hardware approaches. External fixators are frames attached to the bone through the skin using pins or wires, and a mechanical device on the outside of the body drives the lengthening. Internal devices, such as the PRECICE motorized nail, are implanted entirely inside the bone and controlled magnetically from outside the skin. Hybrid systems also exist, combining elements of both. The Cleveland Clinic and International Center for Limb Lengthening both describe this same basic framework, though device types and protocols vary by center and patient anatomy.
The surgery itself has legitimate medical uses: correcting leg-length discrepancies caused by injury, infection, or developmental conditions, and treating specific forms of dwarfism. Cosmetic stature lengthening, meaning surgery on a person with typical proportions who simply wants to be taller, is a separate and more controversial application. Both involve the same bone-cutting mechanics and carry the same biological risks, but the risk-benefit calculation looks very different depending on why you are doing it.
Growth plates, bone age, and why surgery is not a workaround
If your growth plates are still open, you are not done growing on your own, and surgery is almost certainly not the right answer yet. Growth plates, the cartilaginous zones near the ends of long bones, are what actually drive height increases during childhood and adolescence. Most girls reach skeletal maturity around age 14 and most boys around age 16, though individual variation is real and meaningful. A hand and wrist X-ray compared to a reference atlas (the Greulich and Pyle method, for example) gives a bone age assessment that tells a surgeon far more than your birthday does.
Once growth plates close, natural height increase stops. That is the point at which limb-lengthening surgery becomes the only structural way to add stature. For skeletally immature patients with a leg-length discrepancy, a completely different approach, epiphysiodesis, is often preferred instead. Epiphysiodesis deliberately slows or stops growth in the longer leg so the shorter one catches up, and it works only while growth plates are still active. A growth modification approach like this can manage discrepancies of roughly 2 to 5 cm in growing patients, making full lengthening surgery unnecessary for many of them.
The practical takeaway: if you are still in your mid-teens and wondering whether surgery can make you taller, the answer your doctor needs to give you starts with a bone age X-ray, not a surgical consult. If plates are open, non-surgical support (nutrition, sleep, managing underlying health issues) and watchful waiting are the appropriate path. Surgery becomes relevant only when plates are confirmed closed and there is a clear medical or, in some cases, psychosocial indication for the procedure.
The side effects and risks you need to know about

This is the section most people are actually searching for, so let's be direct about it. If you’re looking into height grow powder, it’s important to understand that supplement marketing can’t reproduce the biology of real bone growth. The risks of limb-lengthening surgery span every phase of treatment, and some are serious enough to be permanently life-altering.
Short-term surgical risks
- Infection: Pin-tract infections are among the most common complications with external fixators. The pins pass through skin and soft tissue into bone, creating a chronic entry point for bacteria throughout the months the frame is in place.
- Nerve and vascular injury: Cutting bone and then slowly pulling it apart places constant mechanical stress on nearby nerves and blood vessels. Nerve irritation or partial nerve damage can produce numbness, tingling, weakness, or, in more serious cases, lasting neurological deficits.
- Muscle and tendon tightness: Bones lengthen faster than soft tissues can adapt. The result is progressive muscle tightness, particularly in the calf and hamstrings, which is one of the main reasons physical therapy is required multiple times per week throughout the process.
- Joint stiffness: The Hospital for Special Surgery lists joint stiffness from muscle tension as one of the biggest risks of the entire procedure. If soft tissues contract around a joint, regaining full range of motion can take months of intensive therapy, and full recovery is not guaranteed.
- Swelling and pain: Significant swelling is expected throughout the distraction phase. Pain levels vary, but most patients require structured pain management well beyond what a typical orthopedic surgery involves.
- Blood clots (VTE): Venous thromboembolism, including deep vein thrombosis, is a recognized complication of intramedullary limb-lengthening surgery. Patients typically receive thromboprophylaxis, but the risk is real and is actively managed in reputable programs.
- Scarring: Any surgical incision leaves a scar, and lengthening procedures often require multiple incision sites depending on the hardware used.
Problems specific to the regenerate bone

The new bone that forms in the gap (the regenerate) can fail to mineralize properly. Delayed union means the regenerate is taking longer than expected to harden into solid bone. Nonunion means it may not consolidate at all without further intervention. Premature consolidation is the opposite problem: the gap closes before enough length has been gained, requiring re-osteotomy (another surgical cut) to restart the process. These are not rare scenarios. They are documented reasons why complication rates in the published literature are so high.
What recovery actually looks like, month by month
Most people underestimate how long and disruptive this process is. A full year is a realistic minimum for the bone to be completely healed, and that is for straightforward cases without major complications. Here is a practical breakdown of what the timeline looks like.
- Surgery and latency period (days 1 to roughly 7): The bone is cut during the procedure. A short rest period follows before lengthening begins, typically around 6 to 7 days. During this window the bone starts its initial healing response.
- Distraction phase (weeks 1 to roughly 8 to 16, depending on target length): This is the active lengthening phase. The standard rate is approximately 1 mm per day, often broken into four increments of 0.25 mm each. For every centimeter of height gain, you are spending roughly another week in the distraction phase. Patients use crutches and cannot fully bear weight. Physical therapy sessions multiple times per week are not optional. Pain and muscle tightness are actively managed throughout.
- Consolidation phase (roughly 2 to 4 months after distraction ends): Lengthening stops and the regenerate bone hardens. Weight-bearing is introduced gradually, guided by X-rays taken every 4 to 8 weeks. The external fixation index, a measure of days of fixation per centimeter gained, averages around 15 days per centimeter with modern internal techniques and around 30 days per centimeter with traditional Ilizarov external frames. This phase is often when patients feel most frustrated because the visible work is done but the restrictions continue.
- Hardware removal: External fixators are removed when consolidation is sufficient. Internal nails require a separate surgical procedure for removal.
- Rehabilitation: Even after the hardware is gone, structured rehab continues. Gait retraining, strength work, and flexibility restoration can take additional months. Cedars-Sinai notes that even with intensive therapy, muscle contractures and nerve irritation remain possible complications during and after treatment.
Long-term outcomes, complications, and what 'success' actually means

Published outcomes from cosmetic limb lengthening are generally positive in terms of patient satisfaction, but the picture is more complicated when you look at complication rates honestly. If you are looking for grow taller supplements reviews, be aware that supplements are not a substitute for understanding real surgical risk and outcomes complication rates. A 2021 systematic review of externally controlled motorized intramedullary nails covering 983 segments reported per-segment complication rates of 46% for FITBONE devices and 31% for PRECICE devices. These are not minor issues like temporary soreness. These are tracked complications requiring clinical management.
Residual limb-length inequality above 2 cm, even after treatment intended to correct it, has been associated with lower quality-of-life scores across domains including sleep and pain in long-term follow-up. A limp may persist if gait is not fully rehabilitated or if nerve or muscle damage limits full recovery. Hardware-related problems, including implant failure or malposition, can require revision surgery. The need for a second operation is not unusual in complex cases.
On the positive side, a prospective gait analysis study found that lengthening can normalize stance parameters and eliminate a limp caused by leg-length discrepancy. Patient satisfaction rates in cosmetic lengthening cohorts are frequently high in studies that report them. The honest conclusion is that outcomes are genuinely good for the right patients at high-volume centers with proper rehabilitation, and genuinely risky for everyone else.
| Factor | External Fixator | Internal Nail (e.g., PRECICE) |
|---|---|---|
| Visible hardware | Yes, frame outside the body | No, fully implanted |
| Infection risk | High (pin-tract infections common) | Lower, but still present |
| Complication rate (per segment) | Higher in most comparisons | ~31% (PRECICE cohorts) |
| Fixation index (days/cm) | ~30 days/cm (Ilizarov) | ~15 days/cm (internal techniques) |
| Hardware removal surgery | Frame removal (less invasive) | Separate internal surgery required |
| Patient comfort | Generally lower | Generally higher |
| Cost | Lower in many settings | Higher (implant cost) |
Non-surgical alternatives worth considering first
If you are still growing or if your goal is modest height optimization rather than structural bone change, several evidence-grounded options are worth pursuing seriously before considering any surgical path. None of these will add centimeters after growth plates close, but they can help you reach your genetic ceiling if you are still developing, and they can meaningfully affect how tall you look and feel at any age. If you are looking at grow-taller supplements, make sure they are FDA approved in the Philippines and be cautious with products that make unrealistic claims FDA approved grow taller supplements in the Philippines.
- Sleep: Growth hormone secretion is heavily concentrated in the deep sleep stages, particularly in children and adolescents. Consistently short or disrupted sleep is one of the most modifiable suppressors of growth in younger people.
- Nutrition: Adequate calories, protein, calcium, vitamin D, and zinc are all required for normal bone development. Deficiency in any of these during active growth phases has real consequences for final height.
- Posture and mobility training: While posture cannot change skeletal height after plates close, chronic compression from poor posture, tight hip flexors, or a pronounced anterior pelvic tilt can make a person appear and function shorter than they are. Structured mobility and strength work can address this.
- Medical evaluation for underlying causes: Growth hormone deficiency, thyroid disorders, celiac disease, and other treatable conditions can suppress height gain in children and adolescents. If a young person is growing significantly below expected curves, a pediatric endocrinologist evaluation is the right next step, not a supplement or surgery.
- Supplements: The sibling topics on height growth supplements, powders, and FDA-approved options in various markets are worth reviewing critically. Most lack robust clinical evidence for height gain in healthy individuals, and none replace medical evaluation for genuine growth concerns.
How to decide responsibly if you are still considering surgery
If you have done the research, your growth plates are confirmed closed, and you are still seriously considering limb-lengthening surgery, the decision framework matters as much as the decision itself. Here is how to approach this responsibly.
Questions to ask any surgical program
- What is your center's documented complication rate for this procedure, broken down by complication type? A credible program tracks and shares this.
- How many of these procedures has the lead surgeon personally performed? Volume matters significantly for outcomes in technically demanding orthopedic work.
- What is the full rehabilitation protocol, and is a dedicated physical therapist part of the care team from day one?
- What happens if I develop a complication mid-treatment? Who manages it, and is that covered in the program cost?
- What is the realistic range of height gain for my anatomy, and how is that determined preoperatively?
- What are the criteria for hardware removal, and what does the follow-up schedule look like for the full year post-surgery?
Red flags to watch for
- Any program that downplays complication rates or presents the surgery as low-risk or routine.
- Surgeons who do not perform a formal preoperative assessment including radiographic leg-length measurement, bone quality evaluation, and psychological screening.
- Cosmetic clinics offering limb lengthening without a structured, supervised rehabilitation program built into the care plan.
- Guarantees of specific height gains without discussing the anatomical and biological limits that determine actual outcomes.
- Programs operating in medical tourism contexts where follow-up care after you return home is vague or nonexistent. Complications like delayed union or hardware failure require prompt, local access to a qualified orthopedic team.
- Any provider who seems unfamiliar with the 2024 updated review on motorized internal lengthening protocols or who proposes only older external fixation methods without discussing internal nail options as an alternative.
Finding the right specialist
Look specifically for orthopedic surgeons who specialize in limb reconstruction, not general orthopedic or cosmetic surgeons. Organizations like the Limb Lengthening and Reconstruction Society (LLRS) maintain directories of fellowship-trained specialists. High-volume academic centers, such as those affiliated with hospital systems that publish their outcomes, offer the most transparency. The 2024 updated review on motorized internal limb lengthening explicitly frames the technique as safe and reliable only when paired with sufficient surgeon training and thorough patient education. Both halves of that sentence matter equally.
The bottom line is this: limb-lengthening surgery is real, it works, and for the right patient at the right center, it can produce meaningful and lasting height increases. But the side effect profile is serious, the recovery is long and genuinely disruptive, and the complication rates in published literature are high enough that anyone considering it deserves a fully honest picture before making a decision. Get a bone age assessment, work through every non-surgical option that applies to your situation, and if surgery still makes sense, choose your center based on documented outcomes and transparent communication, not marketing.
FAQ
What are the most common “side effects” people feel day to day during limb-lengthening recovery?
Beyond the headline risks, the everyday issues most patients report include significant pain around the osteotomy period, progressive muscle tightness as the body adapts, and joint stiffness that can make early mobility difficult. Many also experience skin irritation or pin-tract problems with external hardware, and nerve-related symptoms like tingling or burning that may improve slowly but sometimes linger.
How soon can you tell if healing is going off track, like delayed union or premature consolidation?
Surgeons monitor healing with serial X-rays and clinical exam during the distraction phase and after. Warning signs can include longer-than-expected consolidation timelines on imaging, worsening discomfort instead of gradual improvement, or the regenerate appearing less mature than expected. You should ask your surgeon what objective radiographic milestones they use and how often imaging will be scheduled.
Do the side effects differ meaningfully between internal nails, external fixators, and hybrid systems?
Yes. External fixators tend to carry more frequent skin and pin-site complications because the hardware traverses the skin, while internal nails can shift concerns toward issues like nail-related problems, alignment difficulties, and regenerate quality. Hybrid systems introduce the complexity of both, so side-effect patterns can be a mix. The best way to compare is to ask each center what complication pattern they see most often with your specific device and plan.
Will I be able to walk normally, and how does rehabilitation affect long-term results?
Walking can improve, but normal gait usually depends on structured physical therapy and the ability to tolerate lengthening without persistent nerve or muscle limitations. If rehabilitation is delayed or inadequate, residual limp can persist even if bone healing is successful. Ask the team who will supervise gait therapy, how often follow-ups occur, and what rehab protocol they use for your lengthening target.
Can surgery still be considered if my goal is small, like less than 2 to 3 cm?
Often the decision shifts toward alternatives if the discrepancy is small or if you are not fully grown. Because residual inequality and quality-of-life issues can still occur, many patients with modest targets may do better with non-surgical optimization during growth, or with discrepancy-correction strategies that do not require full lengthening. If surgery is still proposed, ask whether the plan is likely to overshoot or undershoot your target and how they plan to manage that.
What is the real chance I will need a second surgery or revision?
Revision risk varies by case complexity, device type, and how closely the regenerate forms as planned. Problems like hardware malposition, alignment issues, regenerate that fails to consolidate, or premature consolidation that requires re-osteotomy can lead to additional operations. A practical step is to ask your surgeon to estimate your personal revision likelihood using their center’s outcomes for similar indications.
How long is recovery in practical terms, not just “bone healing” time?
Bone consolidation can take roughly a year in straightforward situations, but functional recovery often extends beyond that. Many people also need extended time for strength rebuilding, range of motion restoration, and gait retraining, with periodic flare-ups during follow-up adjustments. Ask for an expected timeline for weight-bearing progression, return to school or work, and sports or high-impact activity.
Do nerve symptoms and muscle tightness always resolve?
Not always. Nerve irritation and muscle tightness are common and can improve over months, but the course is variable. Some patients experience persistent altered sensation or ongoing limitations if nerve stretch injury is significant or if the lengthening rate and total distraction amount are not well tolerated. Ask how your team sets the distraction rate, how they detect nerve problems early, and what interventions they use if symptoms worsen.
What should I ask to confirm I am truly a candidate, beyond “are my growth plates closed”?
A useful bone-age assessment (often hand and wrist imaging) should be interpreted alongside your clinical history and leg-length measurements. You should also ask whether there are orthopedic conditions that could change the risk profile, like underlying alignment issues, joint problems, or prior injuries. If growth plates are near closure, the margin of error matters, so ask how your surgeon handles borderline cases.
How can I spot marketing claims that don’t match the actual risk profile?
Be cautious of claims that imply predictable, complication-free “height growth,” or that treat surgery like a short process with minimal disruption. Since complication rates are substantial in the literature and include regenerate and hardware-related problems, any presentation that ignores device type, monitoring schedules, and rehab requirements is a red flag. Ask for specific, center-reported complication categories, not just overall satisfaction.
Next Article
Height Grow Plus Side Effects, Safety, and Does It Work
Evidence-based guide to Height Grow Plus claims, ingredients, real height impact, side effects, safety, and who should a
