Taking testosterone will not make you taller if your growth plates have already closed, which happens for most people by their late teens. If you're an adolescent with open growth plates and a diagnosed hormone deficiency, carefully supervised testosterone therapy might help you reach a more normal final height. But for the vast majority of people asking this question today, exogenous testosterone won't add a single centimeter to your height, and taking it unsupervised carries real health risks.
If I Take Testosterone, Will I Grow Taller? Facts and Next Steps

Marcus Reeves
30 Apr 2026

Testosterone and height: it all comes down to growth plates
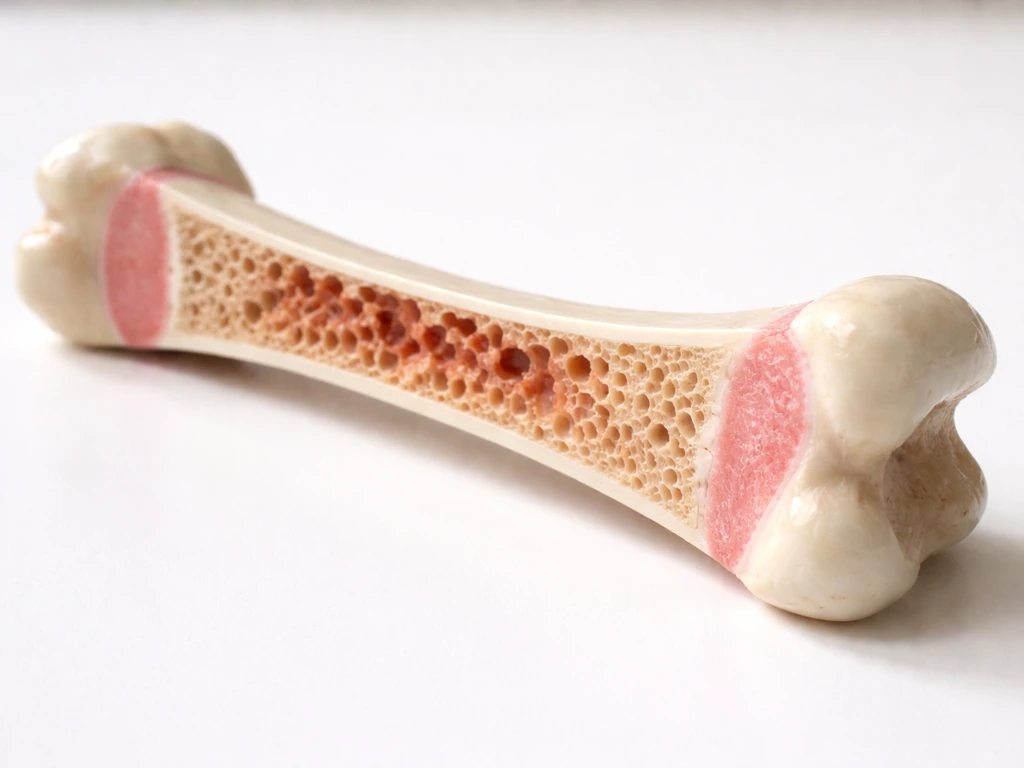
Your height is determined by your growth plates, which are zones of cartilage near the ends of your long bones (the femur, tibia, and others) that allow bones to lengthen during childhood and adolescence. Some people also wonder if wearing bigger shoes makes your feet grow, but your height is still controlled by growth plates, not footwear. These are called epiphyseal plates. Once they fully harden into bone, a process called epiphyseal closure, vertical growth is over. No hormone, supplement, or intervention reverses that. Testosterone's relationship with height is actually a double-edged one: during puberty, rising testosterone drives the growth spurt that can add several inches in a short period, but that same testosterone also accelerates the closure of growth plates. So testosterone is both a growth accelerator and, eventually, a growth stopper.
This is why the question 'if I take testosterone, will I grow taller?' doesn't have a one-size-fits-all answer. The honest answer depends almost entirely on two things: whether your growth plates are still open, and whether you have an underlying condition that has suppressed your natural testosterone below healthy levels.
Adolescence vs adulthood: when testosterone can (and can't) add height
During puberty, testosterone is one of the primary drivers of the adolescent growth spurt in males. Testosterone stimulates the production of growth hormone and IGF-1, both of which act on open growth plates to drive bone lengthening. In a typical male puberty, this spurt can account for 25 to 30 centimeters of height gain over two to three years. So in a physiological sense, yes, testosterone is involved in making adolescents taller. But that's very different from taking supplemental testosterone to get taller.
For adolescents who are in puberty and have naturally rising testosterone levels, their growth plates are responding to the whole hormonal environment of development. If you're a teenager with open growth plates and normal puberty, adding exogenous testosterone on top of that doesn't stack up to more height. In fact, giving excess androgens to a developing adolescent can accelerate growth plate fusion and actually reduce final adult height.
For adults, the situation is straightforward: epiphyseal closure is complete, typically by around age 18 in males and 16 in females, though this varies. Once those plates are closed, there is no mechanism by which testosterone, or any other hormone, can make your bones grow longer. Taking testosterone as an adult will not make you taller, period. If you're asking, “does testosterone make you grow taller,” the key answer is that once growth plates are closed, testosterone cannot lengthen bones.
Medical situations where testosterone might actually help
There are specific, narrow medical scenarios where testosterone therapy in younger patients can support more normal height outcomes. These all involve open growth plates and a clinical deficiency.
Delayed puberty in adolescent males
Boys with constitutional delay of puberty (CDP) or hypogonadism sometimes receive short courses of low-dose testosterone to kick-start pubertal development. The goal here isn't to 'get taller' by adding testosterone; it's to normalize development that is running significantly behind schedule. A JAMA Pediatrics study evaluated a brief course of testosterone enanthate given as four intramuscular injections of 200 mg at three-week intervals in 50 male patients with delayed puberty, measuring effects on pubertal advancement and final adult height. The treatment helped advance puberty, which is the primary aim. However, a separate study in Pediatric Research on boys with delayed puberty found that at the given testosterone dosage, treatment alleviated delayed-puberty issues but showed no significant effect on final height. That's an important finding: even in the medical setting most likely to benefit from testosterone therapy, the effect on final height is modest at best and often not statistically significant.
Hypogonadism with open growth plates
If an adolescent has hypogonadism (clinically low testosterone production) and hasn't yet reached epiphyseal closure, testosterone replacement therapy under medical supervision can help that person develop more normally, including achieving a closer-to-expected height. But this is treatment for a diagnosed deficiency, not height enhancement. The logic is: if your body isn't producing enough testosterone to drive normal puberty, replacement therapy can restore the growth trajectory you would have had. It doesn't add height on top of normal.
Why testosterone won't make most people taller (myths vs evidence)

There's a persistent idea online that testosterone is a kind of growth accelerant you can take to get taller, especially among teenagers who feel they're developing late or who want to speed up their growth spurt. Here's where the science firmly pushes back.
- Myth: Taking testosterone will trigger or extend a growth spurt. Reality: Exogenous testosterone accelerates growth plate fusion. In someone with open plates, it can actually shorten the window of growth, leading to a shorter final height than they would have reached naturally.
- Myth: More testosterone equals more height. Reality: The clinical evidence, including the Pediatric Research study above, shows no significant final height benefit even in boys with delayed puberty who are the most likely to theoretically benefit.
- Myth: Testosterone supplements (boosters) work the same way as prescribed testosterone. Reality: Over-the-counter testosterone boosters are not the same as pharmaceutical testosterone. Most have minimal evidence for meaningfully raising testosterone levels, and none have evidence for increasing height.
- Myth: Adults can still grow if they take testosterone. Reality: Once growth plates are fused, no amount of any hormone changes bone length. This is basic skeletal biology.
- Myth: Trans men who take testosterone will grow taller. Reality: Adults transitioning with testosterone therapy do not experience long bone growth. Adolescents who transition before epiphyseal closure may see some growth changes, but this is a complex, individualized medical situation managed by specialized clinicians.
How to actually figure out your remaining height potential
If you're genuinely trying to understand whether you have height growth left and what might influence it, there are concrete tools and steps for that, and none of them involve self-prescribing testosterone.
Bone age X-ray
A hand and wrist X-ray (sometimes called a skeletal age or bone age study) is the most direct way to assess whether your growth plates are still open. A radiologist compares your growth plate appearance to standard reference images. If your bone age is significantly younger than your chronological age, you likely have growth remaining. If the growth plates appear fused, growth is complete. This is the same test pediatric endocrinologists use when evaluating delayed puberty.
Growth chart tracking
If you've had regular checkups, your doctor likely has height measurements on a growth chart going back years. Plotting these over time tells you whether your growth has slowed or plateaued, which is a strong sign you're approaching or have reached final height. A sudden plateau in height velocity (the rate of growth per year) typically signals that epiphyseal closure is underway.
Pubertal stage assessment
Tanner staging, which describes the five stages of puberty from prepubertal to fully adult, gives a rough indicator of where you are in the growth process. Boys in Tanner stages 2 to 4 typically still have significant growth potential. By Tanner stage 5, most growth is complete.
Lab work
If there's concern about a hormonal issue affecting growth, a doctor can order relevant labs: serum testosterone, LH, FSH, IGF-1, and thyroid hormones are common starting points. Endocrine Society guideline resources for testosterone therapy emphasize diagnosing hypogonadism and distinguishing primary versus secondary causes using LH and FSH, with monitoring for response and adverse effects after starting treatment distinguishing primary vs secondary hypogonadism using LH and FSH. These help identify whether a deficiency is actually present and whether intervention is warranted. Knowing what hormone drives which aspects of growth is useful here, and growth hormone and IGF-1 are actually the primary hormones responsible for long bone growth rather than testosterone directly.
Safety risks and when to see a doctor
This section matters. If you're considering taking testosterone, either from a gym source, online, or even asking a doctor for it specifically to grow taller, there are significant risks you should understand before doing anything.
| Risk | Who it affects most | What happens |
|---|---|---|
| Premature growth plate closure | Adolescents with open growth plates | Can shorten final adult height by fusing plates before full growth is reached |
| Suppression of natural hormone production | Anyone taking exogenous testosterone | The hypothalamic-pituitary-gonadal axis downregulates; natural testosterone production may drop significantly |
| Cardiovascular effects | Teens and adults | Elevated red blood cell count, blood pressure changes, altered lipid profiles with prolonged use |
| Testicular atrophy | Males taking testosterone long-term | Testes shrink due to reduced LH signal; can affect fertility |
| Mood and behavioral effects | Adolescents especially | Aggression, mood swings, and psychological effects are documented, especially in developing brains |
| Injection site complications | Anyone using injectable forms | Infection, abscess, or nerve damage from improper injection technique |
The clearest signal to see a doctor: if you're a teenager who hasn't started puberty by age 14 (males) or 13 (females), or if puberty seems stalled, that warrants a proper evaluation by a pediatric endocrinologist. They can run the right tests, assess your bone age, and determine whether any medical intervention is actually appropriate. Self-prescribing testosterone based on wanting to be taller is not appropriate at any age and carries real risk of harm, including the opposite of what you want for height if you're still growing.
Evidence-based ways to actually support your growth potential
If you have growth remaining (open plates, still in puberty, younger than your mid-to-late teens), there are real levers you can pull that the evidence supports. These aren't magic, but they ensure your body has the best possible conditions to express your genetic height potential.
- Sleep: Growth hormone is secreted in pulses, with the largest pulse occurring during deep sleep, typically within the first few hours of sleep onset. Consistently getting 8 to 10 hours of sleep per night as an adolescent is one of the most concrete things you can do to support GH secretion and growth.
- Nutrition: Adequate protein (around 0.8 to 1.2 grams per kilogram of body weight daily) and sufficient calories are foundational. Deficiencies in zinc, vitamin D, calcium, and iodine are all associated with stunted growth. If you're eating poorly or restrictively, that's a bigger barrier to height than any hormone.
- Treat actual deficiencies: If you're deficient in vitamin D, zinc, or have an undiagnosed thyroid issue, treating that deficiency can genuinely restore growth trajectory. This is different from supplementing on top of normal levels, which typically doesn't add further benefit.
- Physical activity: Weight-bearing exercise and regular activity support healthy bone density and overall development. There's no strong evidence that stretching or specific exercises add height, but staying active supports the hormonal environment (including natural GH release) that supports growth.
- Avoid things that suppress growth: Chronic stress, smoking, excess alcohol, anabolic steroids, and severe caloric restriction all negatively affect growth in developing adolescents. Removing these barriers matters more than adding any supplement.
- Genetics: The honest ceiling. About 60 to 80 percent of final adult height is determined by genetics. Knowing your family height history and using a mid-parental height calculation gives you the most realistic estimate of your target range.
It's worth noting that the question of what hormones most influence height goes beyond testosterone. Growth hormone and IGF-1 are the primary drivers of linear bone growth, and thyroid hormone also plays a critical enabling role. If you're wondering what hormone makes you grow, growth hormone and IGF-1 are the key hormones that drive long-bone lengthening. Testosterone's contribution is real during puberty, but it's one part of a complex hormonal orchestra rather than the main event.
Your practical next step based on where you are right now
Here's a simple decision pathway depending on your situation:
| Your situation | What testosterone will do for height | What you should actually do |
|---|---|---|
| Adult with closed growth plates | Nothing, zero effect on height | Focus on posture, fitness, and evidence-based health. No testosterone needed for height. |
| Teenager in puberty, growing normally | Likely shorten final height by closing plates early | Support natural growth with sleep, nutrition, and activity. Do not take exogenous testosterone. |
| Teenager with significantly delayed puberty | Possibly normalize development if deficiency confirmed | See a pediatric endocrinologist for proper evaluation including bone age X-ray and hormone labs. |
| Adolescent with diagnosed hypogonadism | May support more normal height trajectory under medical care | Follow your endocrinologist's protocol. Do not self-dose or adjust dosage. |
| Unsure of growth plate status | Unknown risk; potentially harmful | Get a bone age X-ray and consult a clinician before doing anything. |
The bottom line is simple: testosterone is not a height-growth tool for most people, and taking it without a clear medical reason and clinical oversight is risky. This is also why the real question is whether testosterone can help only in specific medical cases, not by making your feet grow or adding extra height. If you're in that narrow window where it might matter, a doctor with the right diagnostics is the only path that makes sense. For everyone else, the real work of supporting height potential is much less dramatic than a hormone injection. It's sleep, food, and time.
FAQ
If my growth plates are still open, can testosterone help me grow taller long-term?
Usually no. In the open-plate window, extra testosterone can still advance puberty, and that can shorten the time your growth plates remain active. So even if you get a temporary growth spurt, the more common outcome is earlier plate fusion and no meaningful increase in final adult height.
How can I tell whether I actually have remaining growth before considering any testosterone?
You should not rely on “feeling” like you are growing. The safest practical check is bone age (hand and wrist X-ray), plus a growth chart review (height velocity over time). Labs can help explain why growth is slow, but they do not replace the bone-age decision.
What if I am an adult with low testosterone, would testosterone make me taller?
For adults with closed plates, testosterone does not lengthen bones. If testosterone is prescribed for true hypogonadism, benefits are mainly related to sexual development, bone density, energy, and muscle, not height.
Is it safe to take “low-dose” testosterone from a gym or online to try to get taller?
Yes, it can. Anabolic-androgenic steroid misuse can suppress the body’s own hormones, disrupt normal puberty timing in adolescents, and sometimes affect liver and cholesterol markers. Also, many “online” products are mislabeled, so the dose may be unpredictable even if the goal is “low and safe.”
I’m a teenager and growing slowly, does testosterone still have a chance to add height?
If you are already in late puberty or near Tanner stage 5, the likelihood of meaningful height gain from additional androgens is low, because plate closure is near. In that situation, the most useful medical question is why growth has slowed, for example thyroid status, nutrition, chronic illness, or less common endocrine issues.
If testosterone is not the main driver, what should I ask my doctor to check for height issues?
If you suspect a hormone problem, ask a clinician to evaluate overall growth, not only testosterone. Common starting labs often include IGF-1 (and sometimes IGFBP-3) and thyroid hormones, because growth hormone axis and thyroid status can be the real limiting factors even when testosterone seems “low.”
Can testosterone help boys with delayed puberty reach a better final height?
Not reliably. There are narrow cases where a short, supervised course of testosterone may help initiate puberty in boys with constitutional delay, but studies show that pubertal advancement does not always translate into a statistically clear improvement in final height. The emphasis is development normalization, not height stacking.
What should I do first if I think my testosterone is low and I want to improve my growth?
Do not start or change testosterone before you know your diagnosis. The correct next step is an evaluation by a pediatric endocrinologist, especially if puberty is significantly late or stalled. Stopping or starting hormones without a plan can worsen outcomes by disrupting normal timing and assessment.
Does testosterone affect growth plates through conversion to estrogen?
Testosterone can interact with estrogen through aromatization, which can also accelerate epiphyseal closure. This is another reason more is not better, even when testosterone is prescribed, and why dose and timing matter only under specialist care.
What should I prepare for a doctor visit to figure out whether I can still grow?
The quickest practical “next step” is to book an appointment and bring information your doctor needs: your height history (with dates), pubertal timeline (what age changes started), family heights, and any symptoms like fatigue, weight change, or delayed puberty. That helps determine whether bone age and labs are urgent or whether lifestyle factors are more likely.
Next Article
Does Testosterone Make You Grow? Height vs Muscle Growth
Explains if testosterone increases height or only muscle growth, by life stage, and when to seek evaluation.
