Younger siblings do not automatically grow taller than older ones. In fact, the best available research points in the opposite direction: firstborns tend to be slightly taller on average. A large Swedish study of over 652,000 men found that second-born brothers were about 0.4 cm shorter than firstborns, and third-born brothers were about 0.7 cm shorter. These are small differences, and they do not mean your younger brother is destined to be shorter than you. But they do chip away at the popular idea that younger siblings somehow catch up and surpass their older brothers in height. The real story is more nuanced, and understanding it can help you set realistic expectations for yourself or your child.
Do Younger Siblings Grow Taller? Science and What Helps

Marcus Reeves
1 May 2026

What actually determines how tall someone grows
Height is primarily a genetic outcome. Roughly 60 to 80 percent of your final adult stature is determined by the genes you inherited from both parents. The remaining 20 to 40 percent comes from environmental factors: nutrition, sleep, illness history, and general health during the growing years. Birth order is not a biological mechanism for height on its own. It is a proxy for a cluster of environmental conditions that vary slightly between children in the same family.
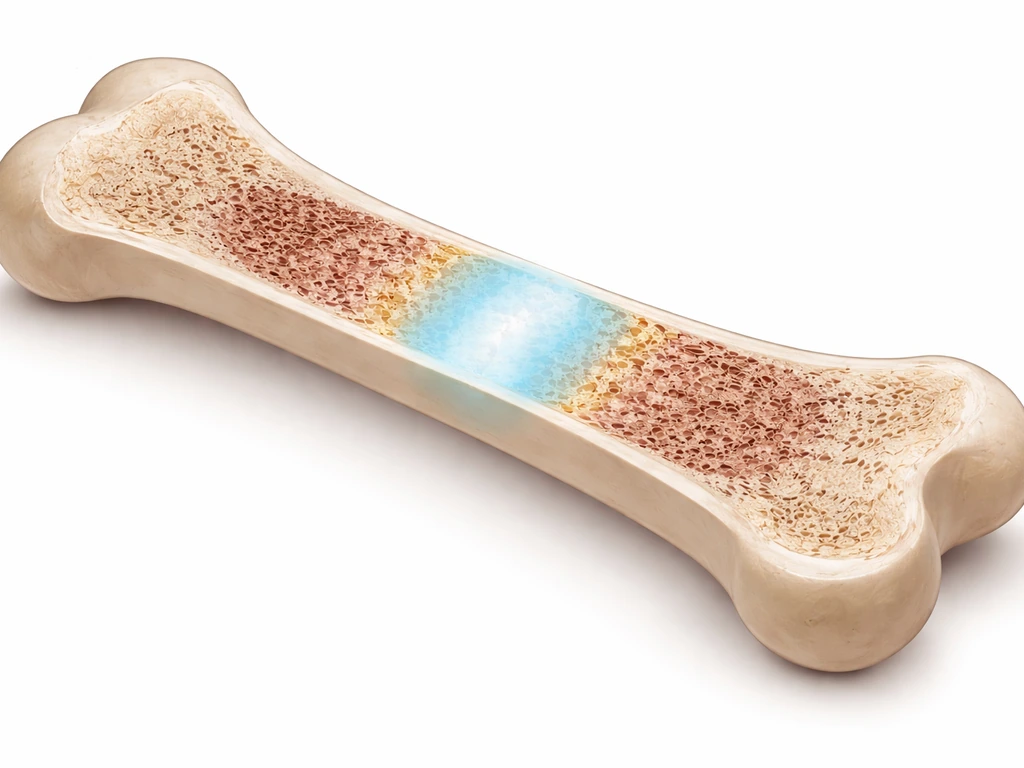
The physical machinery behind height growth is the growth plate, a layer of cartilage near the ends of long bones where new bone tissue is produced through a process called endochondral ossification. Chondrocytes (cartilage cells) in the growth plate proliferate and then enlarge, pushing bones longer. This process is tightly regulated by hormones, particularly growth hormone, IGF-1, and sex steroids.
When sex steroids surge at puberty they initially accelerate growth, then gradually signal the growth plates to fuse and stop producing new bone. Once the plates are fused, linear growth is over. This is why puberty timing matters so much: a child who enters puberty later has a longer window of pre-pubertal growth and sometimes (though not always) ends up taller.
Puberty accounts for roughly 20 percent of final adult height. Boys reach their average peak height velocity around age 13.9 years, gaining close to 9.9 cm per year at the peak. Girls hit peak velocity earlier, around age 12.3 years, with a peak rate of about 8.0 cm per year. Any factor that shifts the timing of this window, whether earlier or later, changes the total height a person adds during adolescence.
Why birth order shows up in height data at all
If genes are shared among siblings and most environmental factors at home are similar, why do firstborns come out slightly taller in large studies? Researchers have identified a few plausible explanations, none of which are dramatic on their own.
Maternal health and the prenatal environment
A first pregnancy is different physiologically from subsequent ones. The uterine environment, placental efficiency, and maternal nutritional stores can all change with each pregnancy. Maternal smoking during pregnancy is a well-documented example: research shows it is associated with reductions in height-for-age z-scores across childhood and adolescence, and later-born children may be exposed differently depending on whether a mother's smoking habits changed between pregnancies. Maternal age, BMI, gestational age, and parity all interact in ways that can subtly shift a child's early growth trajectory.
Early-life nutrition and resource sharing

Firstborn children often receive undivided parental attention and resources during the critical early years. With each additional child, time, money, and food resources get spread more thinly. Early-life nutrition during infancy and toddlerhood is particularly important for linear growth: research on growth faltering shows that inadequate caloric and protein intake in infancy can restrict later height. Breastfeeding duration, illness frequency (more infections are common when older siblings bring pathogens home from school), and early-life stress can all contribute to small differences in growth trajectories.
These effects are real but small
The Swedish research used within-family fixed-effects designs, meaning brothers were compared to each other within the same household, controlling for shared genetics and shared socioeconomic status. Even in that rigorous framework, the height difference between birth orders was less than 1 cm on average. That is a real statistical signal, but it is also well within the range of normal individual variation. Birth order does not override genetics. If you are wondering about how height is shaped for boys over time, it helps to understand the factors behind why can men grow taller.
When a younger brother actually does end up taller
Average trends aside, plenty of younger brothers are taller than their older siblings, and there are legitimate reasons why that happens at the individual level. The most common explanation is puberty timing. If a younger brother starts his growth spurt later than average, he spends more time in the pre-pubertal state, during which he keeps growing at a slower but steady rate before the spurt hits. When his growth spurt finally arrives, it can be larger in magnitude. This pattern is called constitutional delay of growth and puberty, and it is a normal biological variant, not a disorder.
Genetics within a family are not identical copies. Siblings share about 50 percent of their DNA on average, which means the genetic lottery can deal a younger sibling a more favorable hand for height than an older one. A younger brother who inherits height-promoting gene variants from both parents can easily surpass an older sibling who inherited a less favorable combination. No birth-order effect is strong enough to reliably counteract a meaningful genetic advantage.
Lifestyle differences matter too. If a younger sibling has better nutrition, more consistent sleep, or is more physically active during the growing years, those factors can help them express more of their genetic potential. The gap between genetic potential and realized height is real, and environment fills it in.
What you can actually do to support healthy height potential
You cannot change your genes or your birth order, but you can do a reasonable job of making sure nothing avoidable is limiting a child's growth potential. That same logic also explains how K-pop idols can end up growing taller as they move through puberty. The following evidence-based factors are worth taking seriously during the growing years.
Nutrition: the non-negotiable foundation

Adequate protein, calories, calcium, vitamin D, and zinc are the core nutritional requirements for skeletal growth. Children and adolescents need enough total energy to fuel both daily activity and bone elongation. Protein supports IGF-1 production, which is a key driver of growth-plate activity. Calcium and vitamin D directly support bone mineralization. If a child is consistently undereating, even by modest amounts, it can suppress IGF-1 levels and blunt the growth response. This does not mean loading up on supplements; it means making sure meals are balanced and portion sizes are appropriate for age and activity level.
Sleep: when most of the growing actually happens
Growth hormone is secreted in pulses, and the largest pulse happens during deep slow-wave sleep, typically in the first few hours after falling asleep. Chronic sleep deprivation genuinely suppresses growth hormone output. School-age children need 9 to 11 hours per night; teenagers need 8 to 10. This is not a small detail. Consistent, high-quality sleep is one of the most underrated inputs in the height equation.
Physical activity: stimulate, don't stress

Regular physical activity, especially weight-bearing exercise like running, jumping, and sports, stimulates bone formation and supports healthy IGF-1 levels. There is no evidence that normal exercise stunts growth in children. The concern about heavy weightlifting in young adolescents relates to injury risk to open growth plates, not some inherent growth-suppressing effect of resistance training itself. Keeping kids active in age-appropriate ways is clearly beneficial.
Avoid what actively harms growth
Smoking suppresses growth in children exposed to secondhand smoke, and active smoking in adolescents is associated with negative height outcomes. Chronic stress elevates cortisol, which can suppress growth hormone and IGF-1. Alcohol use in adolescence also interferes with hormonal signaling. Keeping the environment as low-stress and substance-free as possible matters more than many parents realize.
How to track growth and set realistic expectations
The most useful tool for understanding a child's growth trajectory is a growth chart. In the United States, providers use WHO growth standards from birth to age 24 months, then switch to CDC growth charts from age 2 onward. The charts display height (and weight) as percentile curves compared to a reference population. A child at the 40th percentile for height is taller than 40 percent of children the same age and sex. What matters more than any single reading is the pattern over time.
A child who tracks consistently along the 25th percentile from age 3 through age 10 is growing normally, even if they are shorter than most peers. A child who drops from the 60th percentile to the 20th percentile over 12 to 18 months is showing a pattern that warrants investigation, because that kind of crossing of major percentile lines suggests something may be interfering with normal growth.
Alongside percentile tracking, growth rate matters. Children typically grow about 5 to 6 cm per year during mid-childhood (roughly ages 4 to 10). Dropping below about 4 cm per year during this window is a flag worth noting. During the pubertal growth spurt, the rate jumps dramatically (up to 9 to 10 cm per year in boys at peak), so context matters: you are not comparing a 13-year-old mid-spurt to a 6-year-old in slow-growth phase.
Mid-parental height is the most practical benchmark for genetic potential. For boys, add both parents' heights in centimeters, add 13 cm, and divide by 2. For girls, add both parents' heights, subtract 13 cm, and divide by 2. This gives a rough target range (plus or minus about 8.5 cm) for where a child is expected to land. If a child's actual trajectory is significantly below that range, that is worth discussing with a doctor.
When to see a doctor and what to ask
Most height variation between siblings is completely normal and does not require medical evaluation. But there are situations where a doctor visit is genuinely warranted.
- A child's height is below the 3rd to 5th percentile consistently over time
- Growth rate has slowed significantly and the child is crossing percentile lines downward
- A boy shows no signs of puberty (no testicular enlargement) by age 14, or a girl shows no breast development by age 13
- A child's height is well below the range predicted by mid-parental height
- There are other symptoms like fatigue, weight changes, chronic illness, or poor appetite alongside slow growth
When you see a pediatrician or pediatric endocrinologist, they will review your child's growth chart pattern, family history (including what age parents and siblings went through puberty), and medical history. They may order a [bone age X-ray](https://www. ncbi. nlm.
nih. gov/sites/books/NBK596800/), which compares the maturity of growth plates in the wrist to expected levels for a child's age. A bone age that is younger than chronological age often signals constitutional delay, meaning the child will likely catch up given more time. Astronauts may experience changes in height in space because long-term exposure to microgravity can affect how the spine and other tissues bear load bone age.
Blood tests can check thyroid function, IGF-1 levels, and other hormonal markers if there is clinical concern. The Endocrine Society emphasizes that most underlying causes of true short stature are medical (thyroid disorders, growth hormone deficiency, chronic illness) rather than anything related to birth order or sibling dynamics.
Questions worth asking at the appointment: What percentile is my child tracking on, and has that changed? What is their bone age compared to their actual age? Is their growth rate normal for their pubertal stage? Is there anything in the family history I should factor in? These questions move the conversation toward actionable information rather than vague reassurance.
The bottom line on birth order and height
Birth order has a measurable but very small association with adult height, and the data suggests firstborns have a slight advantage, not later-borns. The idea that younger siblings naturally grow taller is a myth when applied as a universal rule. Do short people grow taller? In many cases, their growth is simply reflecting normal genetics, nutrition, sleep, and puberty timing.
What actually determines whether a younger brother ends up taller than his older sibling is the same thing that determines height for any individual: the genetic cards they were dealt, how well their nutritional and sleep needs were met during childhood and adolescence, and how their puberty timing played out. If you are wondering whether factors like a future Mars mission could change height, remember that adult stature is still mostly shaped by genetics, nutrition, sleep, and puberty timing.
Men and women can differ in average adult height mainly because of differences in puberty timing and sex hormones. For most adults, height is largely determined by genetics and how well growth needs were met during childhood and adolescence, so it is not usually something that can be changed after the growth plates fuse adult height.
If you are a younger sibling wondering about your own height ceiling, your parents' heights and your current growth trajectory are far more informative than your birth order. And if you are a parent tracking a younger child who seems behind, consistent monitoring with a growth chart and an honest conversation with your pediatrician will tell you far more than any sibling comparison.
FAQ
If younger siblings do not catch up by birth order, how can a younger brother end up taller?
In many families the effect of being “younger” is really about timing of puberty and early growth, not a catch-up rule. If your growth spurts later than average, you can end up taller even if you started shorter, because you had more time for gradual pre-pubertal growth before the bigger spurt.
Can I estimate my adult height based on whether I am the second, third, or later child?
No. You cannot reliably predict adult height from birth order, especially when the average birth-order differences in large studies are under 1 cm. For a more accurate estimate, use growth-chart trend plus mid-parental height and (for boys and girls) note whether they are early, on-time, or delayed for puberty.
What growth-chart pattern is most concerning, and what is normal to ignore?
A growth chart can look “normal” even when a child is shorter than peers, if the line stays parallel over time. What is more concerning is a sustained drop across percentile bands (for example, crossing multiple major percentiles) or a growth velocity that falls below the expected range for that age and pubertal stage.
Why can two brothers with similar genetics end up with very different heights?
Yes, indirectly. Even if you share the same home, siblings can have different exposures to illness frequency, school schedules, sports participation, sleep duration, and diet quality. Those environmental differences can widen or narrow the height gap enough that real outcomes do not match the small average birth-order trend.
If nutrition is important, should I give my child height supplements to help them grow?
Supplements help only when there is a deficiency or clear inadequate intake. If a child eats poorly, a “complete” supplement may not fix the underlying problem, and too much of certain nutrients can be harmful. A clinician may check vitamin D or other labs only if there are reasons to suspect deficiency or a failure to thrive pattern.
Does playing sports or lifting weights stunt growth?
Not usually. Regular age-appropriate exercise supports healthy growth and bone development. The main risk with heavy resistance training in early adolescence is injury to growth plates or technique-related problems, not a permanent growth-halting effect from exercise itself.
If my child gets enough hours of sleep, can sleep still affect height?
Breathing and sleep quality matter. Conditions that fragment sleep, such as sleep apnea, can reduce deep slow-wave sleep and thereby reduce growth hormone pulses. If snoring, witnessed breathing pauses, or severe restless sleep are present, it is worth discussing with a pediatrician.
Why does puberty timing matter more than current height when comparing siblings?
Puberty timing can shift the total height gained, especially because the growth spurt is tied to sex-steroid changes that also signal growth plate closure. Two kids of the same age can be in different stages of puberty, so “who is taller right now” is less informative than growth rate relative to pubertal stage.
When would a pediatrician order a bone age or lab tests for suspected short stature?
Doctors usually look for three things: growth chart trajectory, growth velocity, and possible hormonal or medical contributors. A bone-age X-ray is most useful when there is a mismatch between chronological age and skeletal maturity, such as consistent slowing or suspected constitutional delay, endocrine issues, or chronic illness.
If a child’s height target is lower than expected, how do we know it is normal familial pattern versus a medical problem?
Mid-parental height gives a rough target range, but it is not a verdict. If a child’s growth is tracking along their own curve and family members had similar timing (for example, a parent who matured late), that can explain shorter stature without disease. The key is whether growth velocity and percentiles are staying stable rather than abruptly declining.
Next Article
Can Adults Grow Taller? What’s Possible and What Helps
Can adults grow taller? Learn what’s biologically possible and what helps height via posture, mobility, and lifestyle.
